Story
 August 31, 2024
August 31, 2024
Choking to Death: Silica Dust from India’s Industries Is Killing Its Workers
Country:


Silicosis is a fatal lung disease that affects millions of Indian mining workers.

I
MILAN PATRA was 22 years old when he moved to Jharkhand, in around 2016. He hailed from a poor family in the Rai Paria village of Jhargram district, in the Jangalmahal region in West Bengal. Patra had never received an education, and there were no opportunities for work around his village. Like many others in the area, he travelled several hundred kilometres away from home to work, as a daily-wage labourer at a ramming-mass factory in Jharkhand. Ramming mass is a type of powder compound used to line furnaces in steel factories. Patra’s job was to fill the powder into sacks and to load them into storage.
In less than a year, he fell seriously ill. He developed breathing troubles and a nasty, persistent, cough. He was always exhausted, finding it difficult to get through even a few hours of work. He began losing weight. Patra was scared—workers often discussed among themselves stories of colleagues who developed breathing troubles and left, never to return. Many, they had heard, died of their illness. Fearing for his life, he decided to leave his job and return to his village. There was no hospital nearby but he travelled to some health centres in the district, where he was diagnosed with tuberculosis and prescribed medicines for his condition.
The family’s circumstances were precarious. Patra was the only earning member, and his aged parents, as well as his wife and two-year-old son, depended on him. After he fell sick, they struggled to survive, unable to manage two meals a day. The tuberculosis treatment was not helping, and his condition only worsened. It soon became near impossible for him to talk without gasping for breath, let alone to walk or work. When he approached the health centres again, he was given some shocking news. They told Patra that he did not have tuberculosis. He had a condition called silicosis, a lung disease caused by inhaling particles of active silica dust, or silicon dioxide—a major component of ramming mass.
Part of:


Unlike tuberculosis, silicosis was fatal and incurable, although Patra was not aware of this. In early 2020, the family borrowed money from its relatives and friends in the village and made its way to the national capital. Patra was hopeful that he would be able to get better treatment at the renowned All India Institute of Medical Sciences.
But there was another shock in store for the family. In late March, the government declared a sudden lockdown owing to rising cases of COVID-19 across the world. Like millions of other migrant workers, Patra, his wife and son were stuck in the city. Worse, the outpatient department at AIIMS shut down indefinitely, dashing his hopes of recovery. The family spent whatever little money it had on a homeward journey for Patra’s wife and son, leaving him sick and helpless in the city.
I spoke to Patra over the phone during this time, while reporting on the disastrous consequences of the sudden lockdown on migrant workers. He could not complete a full sentence without pausing. His voice was raspy, breathless. He was desperate for help. Patra sent me his medical documents, thinking that I may be able to help him with his illness. He did not think that he would die soon but was aware that his future was bleak. “I know people who died of this problem,” he told me, sounding fearful. He said that some citizen do-gooders were helping him with funds so that he could travel home.
He returned home to Jhargram in June 2020. Treatment was out of the question—he did not have the funds, and the shutdowns caused by the pandemic had pushed the nearly inaccessible healthcare systems further out of reach for him. Besides, few doctors in Jhargram knew what silicosis was. Patra suffered at home, bedridden and helpless. He died in December 2022. He was 28 at the time.
SILICOSIS IS likely the most underreported occupational disease in India. Often called the “grinder’s asthma” or “miner’s phthisis,” the disease is caused by continuous inhalation of active silica dust particles, which are smaller than five microns and invisible to the naked eye. It is most common among workers in industries that involve direct exposure to silica dust—one of the most commonly occurring minerals in the earth’s crust—such as mining; quarrying, cutting, grinding, carving and polishing of stones; manufacturing of construction materials; foundry; glass; and ceramics. Indian industries where silicosis is common include slate-making, agate stone and imitation jewellery, and temple stone-carving.

Silica dust causes the formation of fibrous nodules and scarring inside the patient’s lungs that make it progressively harder for oxygen to enter, slowly choking them to death. Geeta, a widow I met in the Lalkuan region in the national capital, told me that at the time of her husband’s death, silicosis had made his lungs “solid as a stone.” Residents of villages in Madhya Pradesh described how, owing to the fibrous growth, victims’ lungs would not burn easily even in cremation fires.
The scale of the silicosis crisis in India is staggering. A report by the Indian Council of Medical Research in 1999 estimated that, apart from 5.4 million construction workers, three million workers in other industries were at high risk of silica exposure. These figures are already over two decades old, but exact current estimates are near impossible to come by—there have been no national efforts to study the disease, and the onus of documenting it has fallen on activists, medical researchers or victims themselves. But estimates by researchers I spoke to suggest that the number of Indian workers exposed to silica dust and, therefore, at great risk of contracting silicosis, will touch 52 million by 2025. By all counts, it is one of India’s most urgent public-health emergencies.
But even more staggering than the scale of the crisis was how completely uncharted it is. Over the course of the past two years, I travelled to 12 states: Rajasthan, Gujarat, Haryana, Uttar Pradesh, Madhya Pradesh, Jharkhand, West Bengal, Uttarakhand, Tamil Nadu, Andhra Pradesh, Telangana and Karnataka. I visited close to two hundred villages, as well as several towns and cities.
The crisis I witnessed seems far greater than what has been reflected in any official figures so far. I met five hundred families who had been affected by the disease, and who had lost at least one family member to it. I also spoke to dozens of activists and experts who have been working on the silicosis crisis in their respective states. My reporting suggested that the disease has been an invisible killer for decades, and that its death toll in post-Independence India must already be in the millions. But hardly any mentions of silicosis can be found in government policy, nor is there any national-level data on its prevalence. In fact, no state I visited had any accurate record of silicosis victims.

Victims of silicosis, such as Patra, were often misdiagnosed with tuberculosis. The two diseases are not medically similar in any way—tuberculosis is an infectious disease that spreads when a patient coughs, sneezes or talks, releasing bacteria droplets in the air. The misdiagnosis happens not only because symptoms overlap but because doctors remain woefully unaware of silicosis. Several physicians I met knew little more than the textbook definition of the disease, and struggled to explain its details. When I spoke to Patra, it was the first I had heard of silicosis too, and most journalists I spoke to had never heard of the disease, either.
Like Patra, even the victims I met had no idea they were suffering from the disease. In one village in Madhya Pradesh, I met Thawari Munia, a Bhil woman whose five sons and three daughters-in-law, all in their twenties or thirties, too had succumbed to what was described to me as a mysterious illness of the lungs. Her husband, too, had died of the same disease. In her village, they simply called it “Godhra ki beemari”—the illness from Godhra, because the Adivasi residents in the area travelled to Godhra in Gujarat to work in ramming-mass or quartz-grinding factories only to come back sick, and die.
In a handful of states, such as Rajasthan and West Bengal, strong people’s movements against silicosis led to marginal improvement in awareness among public doctors, or to a government policy for compensation and healthcare support for victims. The National Commission for Human Rights too has repeatedly notified states and directed them to carry out regular screenings and establish prevention and compensation regulations. But facilities for regular screening are either absent or sorely lacking, especially in rural areas. Many of the victims I came across were never screened, let alone diagnosed. Many factories or mines where these people worked are either unregistered or illegal. A huge section of the workers are not listed as formal employees, making them ineligible for even the basic labour protections codified in Indian law, such as employees’ insurance.
Even the most progressive policies focussed only on compensation and not prevention or accountability. Public discourse on silicosis is largely non-existent, as are any government efforts to hold industries accountable for their failure to protect their workers from contracting the disease. Its reckoning as a public-health crisis remains pending largely because the people it affects—the poor workers of the very industries that undergird the Indian economy—are already invisible to the system.

No one thing, I found, had damned the victims more than the accident of their birth. Most affected families I met were from Adivasi or oppressed-caste communities. They were born into and lived in abject poverty, with little or no land holdings, and were often forced to migrate for work. They were largely employed in the unorganised sector, where they worked without any protective gear, and were exposed to hazardous dust for hours at a time, for days on end, year after year, for as little as Rs 150 a day.
Afraid to lose their source of income, many hid their illnesses and worked for as long as possible, continuing their exposure. Once they fell too sick to work, they travelled back to their villages, spending their remaining days waiting to die. If they were lucky, they would get help from some activist organisations to access oxygen support to help elongate their life a little, or to get some compensation or insurance under government schemes. Often, their relatives would take their place at the jobs, creating a vicious, generational cycle.
In the villages of Jhabua, in Madhya Pradesh, I met close to two hundred victims in two days—people had travelled from nearby villages when they heard someone from Delhi had come, just to show me their documents in the hope that I could help in some way. This desperation was all too common in my reporting.
GN Devy, a linguistics scholar who has spent his career working with Adivasi communities in Gujarat and Madhya Pradesh, told me that he had witnessed this pattern during his work as well. He said silicosis was among the main afflictions that had besieged Adivasi workers, terming it “a human tragedy on an epidemic scale.” Public-health infrastructure, he said, was almost non-existent in those tribal towns. “The factory owners had not made any insurance provision for them,” Devy said. “Unscrupulous labour contractors were busy inducting more and more young adults in the hard labour occupations pushing to more of the unsuspecting victims towards this death by choked lungs.”


“The situation was alarming, tragic and infuriating,” Devy added. “Adivasis of India, already groaning under a trans-generational debt burden, became its hapless victims. The disease was not just a medical issue, but a deeply political and economic one.”
Lacchu, a Gond man residing in Bador, a village in Madhya Pradesh’s Panna district, had spent most of his life working in the mines near his village. Lacchu was in his forties. He had initially been diagnosed with tuberculosis, but after a few years and a round of failed treatment, doctors in Panna deduced he had silicosis. He had managed to get some medicines under the Ayushman Bharat scheme, but was struggling to make ends meet. He had taken a loan of Rs 50,000 to be able to continue some treatment to manage his symptoms. After his case was covered in a local newspaper during election season, some members from the campaign team of the area’s parliamentarian arranged for five kilograms of wheat, about two kilograms of dal, and Rs 1,000 for him, but that is all the help he got. “I have no money and I need some financial help from the government—whatever a silicosis patient gets,” he told me. “When I ask for that, doctors say I will get money after my death. What is the use of that money after death if I need it now for the treatment?”
II
JAGANNATH PATAR was confined to a bed in a ward at MGM Medical College in Jamshedpur, in Jharkhand. He was emaciated—I could count the ribs on his body. Patar required 24-hour oxygen support to stay alive. When I went to visit him in August last year, he could barely speak for breathlessness. But the 33-year-old had a unique request: He was craving some sweets. Patar asked Samit Kumar Carr, an activist who had taken me to meet Patar, to bring him some. Carr did, but Patar did not eat much. He was not able to remove his oxygen mask for more than a few seconds.
Patar had worked for close to a decade in the ramming-mass industry in Dhalbhumgarh, in Jharkhand’s East Singhbhum district. He was involved in the grinding and milling of quartz and, therefore, inhaled high quantities of silica. Within a couple of years, Patar developed breathing troubles and a dry cough. He rapidly lost weight. He visited some local doctors—from what I gathered, these were not qualified professionals, but small clinics or quacks. For the next several years, he continued to work, taking medicines to ease his symptoms. He was never screened for silicosis at any medical facility nor at his place of work, but he did undergo some treatment for tuberculosis. Eventually, his disease progressed, and he was forced to stay home. It soon became impossible for him to breathe without external oxygen support.

He was finally diagnosed with silicosis nine years after he first fell sick, in 2022, with the help of Carr, who heads an NGO named Occupational Safety and Health Association of Jharkhand. OSHAJ works primarily with victims of silicosis in the state, helping them seek treatment and compensation from the government. OSHAJ had helped Patar get screened and diagnosed, and also helped him with admission at MGM. The screening found that he had tuberculosis as well, but it was unclear when he had developed it. Under a Jharkhand government scheme for silicosis victims, Patar received Rs 1 lakh for his treatment, which soon ran out, owing to his medical bills. He was not aware that the disease could not be cured. Carr had assured Patar that the doctors would release him when they could, but this was said just to ease his distress. Patar was on his deathbed.

Other workers I met had the knowledge that their days were numbered. Bhandha Sabar worked as a daily-wager at a factory in Jharkhand for five years. The main products this factory produced were quartz powder and ramming mass. He fell sick in 2016. He too developed breathing issues and a dry cough, and was forced to leave his job. Sabar said that over one hundred and fifty men worked at the same factory as him, many of whom, like him, were from Adivasi communities. A large number of his co-workers had died from silicosis, he said. “Either today or tomorrow, I am also going to die,” he told me when I met him in September last year. “I just want my family to be okay.”
Many of the silicosis victims I met had contracted the disease away from home. For instance, 45-year-old Rajjak Molla never thought that migrating to earn more than the sixty rupees a day he made working in his village would cost him his life. Molla and his family left their West Bengal village of Goaldaha, in North 24 Parganas district, in 2005, for work. “I chose to work in a stone factory and was getting a hundred and fifty to two hundred rupees. It attracted me, and others too,” Molla told me. “We were in such a bad financial state in the village that we never thought about the consequences of the work. All of us migrated, but I gradually started having breathing issues and sometimes fever, which was detected as TB.” Molla and his family members left the jobs and returned to West Bengal, where they were diagnosed with silicosis. Five of his relatives had died. He and his brother, both in their early thirties, were also suffering from the disease.


If these accounts sound repetitive, it is because they were. Reporting the stories of silicosis victims was like watching the same horror film over and over again, one whose ending you knew all too well. Patar died six months after I met him, in April this year. Sabar died in July. The ones who survived had few avenues to seek even palliative care.
Ramdev Jatav, a resident of the Karauli area in Rajasthan, developed silicosis in his mid-thirties, owing to nearly two decades of consistent exposure to silica dust at a stone quarry. Unlike ramming mass, which is more than ninety-percent silica dust, stones at quarries have anywhere between thirty and seventy percent. Workers at such quarries or mines fall sick slowly but surely, after many years of continuous exposure. When I met him in April this year, Ramdev was in the final stages of the disease, and was bedridden. “For the past few months, I have been facing acute breathing issues, and that is why I have to use an oxygen concentrator,” he said, in between those telltale rasping breaths. The home oxygen support system was not entirely reliable because of electricity shortages. During long power cuts, he would get admitted to a hospital. “So, this is my life now—a burden to my family, at this age,” he said.
Ramdev’s wife, Sunita, began crying while talking to me. She was worried for her son, who had left his studies and taken up a job at the mine. “If the father is sick and bedridden, what will the kids do?” she told me. “They have no choice. At a young age, they can get a job nearby, and mines are the easy option.” Sunita was worried about the family’s financial situation as well. “What we received as compensation, Rs 3 lakh, we spent on the marriage of our two daughters and on repaying the loans we had taken for my husband’s treatment, since we’re poor,” she said.
Ramdev and Sunita reside in Kosra, a village in Rajasthan’s Karauli region that is home to many Dalit families. Like them, most villagers are employed in the nearby stone mines. Several of Ramdev’s family members reside in the village. His younger brother, Dayaram, who is in his late twenties, works in the mines as well, despite knowing that he could get silicosis like his elder brother. “Poverty is the factor that compels us to go for such work,” Dayaram’s wife, Asha, told me. “No other options for livelihood are available here, so people go to the mines.”

Karauli is filled with silicosis victims like Ramdev, ranging from people in their thirties to those in their seventies. All of them had a history of working in mines for anywhere between ten and forty years. They were all dependent on oxygen support, and needed help to be able to afford it. Raju Pal, a 60-year-old resident of Mamchari village, alternated between a nebuliser, an inhaler and an oxygen concentrator. He had to pause between taking a bath and wearing his vest, just to take in some oxygen. Like Ramdev, Pal’s son too had taken up a job at the mines. Pal had received Rs 1 lakh compensation from the Rajasthan government. “I don’t know how much time I have. I would have died two years ago without oxygen support,” he said. “I am only worried about what will happen to the family after me.”
Countless workers I met, such as Jitendrabhai Narayanbhai Parmar, a 66-year-old silicosis patient from Thangadh, in Gujarat, were stuck in a bureaucratic nightmare. The Thangadh and Morbi regions in the state are the ceramic hubs of India. By industry estimates, the ceramic business has a turnover of close to Rs 20,000 crore on the lower end, and there are close to one thousand manufacturing units in Morbi alone. Products manufactured in this region—wall tiles, floor tiles, bathroom tiles, sanitary ware, glazed porcelain, ceramic houseware—are present in nearly every building of the country.
Parmar had worked in the ceramic industry in Gujarat for the better part of thirty years, doing glazing work. He fell sick in 1998, and was compelled to leave his job by 2005. He was only diagnosed with silicosis in 2017, and officially certified as a silicosis patient in 2022. When I met him at his home, he brought out an old photograph of himself from the early 2000s, to show me how much weight he had lost due to his illness. “I was 64 kgs in 2004,” he told me, his voice low and sad. “I am only 31 kgs now.”
Parmar was still luckier than most workers I met. Factories in Thangadh were largely formally registered and subject to labour laws and protections, making Parmar eligible for benefits under the Employee State Insurance Act, 1948—a social-security legislation that offers insurance cover to workers who develop occupational diseases. But his luck ended there. Even though the government had been deducting a portion of his salary every year, now that he was sick, he was not able to claim any insurance payout. “My financial condition is not good and I am dependent on medicines from the government hospital,” he said.

“My ESI was deducted for 15 years and I have all the documents,” he told me, bringing them out. “I got nothing from the company, ESI or the government.” He had been following up with various government bodies since he was officially diagnosed, he said, but had not received any response. Parmar died in June.
While silicosis is an occupational disease that affects individuals, the devastating and longstanding effects it has on entire families cannot be captured by simply recording the death toll. I visited several villages across India populated by women who are referred to as “silicosis widows”—women whose husbands had worked in mines or stone-work industries and lost their lives to the disease. Madauna village in Uttar Pradesh’s Lalitpur district was a collection of mud huts with makeshift roofs made of twigs and leaves. Most of the children milling about showed visible signs of malnutrition. The residents of the village hailed from the Saharia tribe and worked in mines close to their village. Groups of women were huddled at the end of the road leading to the village, waiting to speak to me. They had all lost their husbands and sons to silicosis, although they did not know what the disease was called. Halkibai, one of the widows, had lost her husband to a lung disease, which he developed after working in the mines for many years. She told me she was struggling to earn enough to support her family. She has two sons. One is blind and unable to work. The other son worked in the mines for many years and is now showing symptoms of advanced silicosis.
In Gujarat, I met Rizvana and Khushboo Gori, two cousins from the Dhrangadhra town in Surendranagar district, who had married two brothers, Hamid and Farukh. The brothers worked as stone-carvers since childhood. The two eventually contracted silicosis, although they were never officially diagnosed, and had been receiving treatment for tuberculosis for years. Hamid died at the age of 40, and Farukh at the age of 37. Their mother, Noorjahan, told me that her husband, also a stone-carver, had died early as well. “If we were aware of the disease caused by working in stone-carving, then we would have never gone for these marriages,” Khushboo told me.

I met close to fifty women in the villages of Gandhi Gram and Manor, the “widow villages” of Panna district, who had similar stories. In Elkatta village in Telangana’s Ranga Reddy district, several women told me their husbands had died young after working in quartz mines. They repeated the same symptoms: breathlessness, cough and vomiting blood. The women called it “guttala bimari”—a sweet disease. At the end of every workday, the mine workers were given a piece of jaggery to eat. Mine owners told them that the jaggery would help protect them from the dust they were inhaling.
III
THE PROCESS OF DIAGNOSING SILICOSIS is fairly basic. Since the disease can only be caused by exposure to silica dust, an occupational history of work in at-risk industries is the surest indicator. Most often, this can be combined with a series of chest scans and a sputum test to rule out other infectious diseases, to arrive at a reliable diagnosis.
The World Health Organisation and the International Labour Organization have determined a global standard to diagnose silicosis. “The ILO has devised a set of 23 standardised X-ray plates and its user manual for objective rating of chest X-ray plates of the persons exposed to active dust,” Kunal Dutta, a physician from West Bengal who is an expert in respiratory and occupational diseases, explained. “This rating, when done by three independent readers, is accepted internationally as the standard method of identification of dust-related occupational lung disease, including silicosis.”
But even this straightforward procedure is not implemented in most of India. In Rajasthan, after movements by activist organisations, the state’s human-rights commission issued guidelines to government hospitals to train doctors in early detection of silicosis using the ILO plates. But the decision, taken in 2013, is yet to be enforced. “This is in spite of the fact that in 1995, the ILO and WHO jointly started a global programme to eliminate silicosis by 2030—even these organisations do not seem to be serious about the matter,” MK Devarajan, a former director general of the Rajasthan Police, who was a member of the state’s human-rights commission for several years, told me. Rajasthan accounts for the country’s highest number of silicosis cases each year, which, Devarajan said, was only because it was detecting and documenting silicosis more sincerely than others.
Dutta said that the medical fraternity simply did not know enough about silicosis. “Occupational health is not given importance in medical curriculum in India because it is related the most to those who are poor, the labourers,” he told me. “So, the subject is not taken on priority to teach and train future doctors in a way that they could correctly diagnose occupational diseases like silicosis or even other such pneumoconiosis conditions”—the family of lung diseases such as silicosis and asbestosis.
What Dutta described was a systemic indifference towards silicosis and its victims. “In practice, the doctors take least interest in such diseases of the poor because it is not a subject of profit,” he said. The infrastructure to train doctors, he added, was inadequate. That is why, several experts told me, doctors regularly misdiagnosed silicosis as tuberculosis. In dozens of families I met, the failure to diagnose silicosis had a generational impact—many had died unknowingly of the disease, thinking they had tuberculosis or some other unknown condition, while others would often return to work while receiving treatment for the wrong disease, continuing their exposure to silica dust and worsening their health.
Devarajan echoed Dutta. “Except for some specialists, the general medical fraternity had insufficient knowledge about the disease, how to detect it and how to confirm their diagnosis,” he told me. “This resulted in the doctors of our PHCs and CHCs”—primary and community health centres—“making wrong diagnosis of silicosis as TB and treating the patients for TB, which further resulted in the deterioration of the disease.” In the handful of states that have policies for silicosis relief, misdiagnosis also means that victims are deprived of the silicosis-related compensation owed to them.
The failure to diagnose silicosis, and the confusion with tuberculosis, reveals the central flaw at the heart of India’s public-health priorities. India simply has not invested resources into infrastructure to screen and diagnose the millions of poor workers who are dying of silicosis. In West Bengal, for instance, Dutta told me, only two centres are designated to officially diagnose occupational diseases. “Despite the intervention by the NHRC and the pronouncement of a silicosis intervention plan by the state government, no testing or diagnosis facilities exist under health department in our state as yet, to my knowledge.” Volunteers and civil-society organisations had set up one centre for diagnosing occupational diseases, he said, and another was coming up. But it does not take an expert to know that these are too few centres for a state where hundreds of thousands, if not more, work in at-risk occupations.
Several activists I spoke to, across multiple states, said that, besides being unaware and indifferent, government doctors and institutions actively suppressed silicosis cases to help governments escape accountability. If their factories fell under the Employees’ State Insurance Act—which many, being in the unorganised sector, do not—workers were also eligible to make an insurance claim to cover some of their medical bills, but government doctors were often reluctant to formally write down silicosis as a diagnosis. “Notification is not done and doctors generally diagnose the workers as TB patients. This way both the system and the employer get an exemption from the legal process and also the compensation,” Dunu Roy, an activist from Delhi, said. “These things are against the poor workers and need to be addressed properly.”
Sameena Yusuf, who runs the Prithvi Trust, an NGO that works with silicosis victims among mine workers in Madhya Pradesh’s Bundelkhand area, told me that she had found doctors were reluctant to send patients for a silicosis test and would usually only recommend a CT scan. Even this was a hurdle for many mine workers. “If a labourer has an Ayushman card, the test is free and, if not, then he or she has to pay Rs 1,100 for the test,” she told me. “I found that most of the workers don’t have an Ayushman card and so they find it difficult to pay Rs 1,100 for the test. In that case, they skip the test. That test is never done, and we do not get the actual data of silicosis in the area.”
Her organisation has been working to help silicosis victims get government certification. In 2012, Prithvi Trust had identified 162 victims in Panna district. “We fought for the certification of silicosis cases but managed to get only 46 cases certified by the government, in which 26 have died till now,” Yusuf told me. “We again fought for the financial and social rehabilitation for the dead people, but only 18 got the financial assistance as relief fund as per the policy and eight cases are still pending.” Yusuf had then helped the families approach the NHRC for compensation.
Carr told me that OSHAJ often organised screening camps for at-risk workers with the help of volunteer doctors, using the ILO rating systems. “But that report is not valid for the system, and hence we ask the system to check them once. It is a complex and tough task.” In his experience, he said, doctors felt pressured not to certify silicosis cases, since that would increase the number of people who became eligible for compensation and relief. “The system does not want to write the word ‘silicosis,’” he said.
THE CONFUSION WITH TUBERCULOSIS is a double-edged sword. India has the world’s largest burden of tuberculosis. The Narendra Modi government declared, in 2018, that it would end tuberculosis in the country by 2025. This deadline is doomed to be missed for many reasons, but its failure is also intertwined with India’s inability to recognise and prevent silicosis. Predictably, misdiagnosing silicosis as tuberculosis increases the burden of the latter disease. But, more importantly, silicosis victims are, in fact, more susceptible to tuberculosis—some experts suggest that silica-exposed workers are more than seven times more likely to contract tuberculosis.

Kamalesh Sarkar, the former director of the Indian Council for Medical Research’s National Institute for Occupational Health in Ahmedabad, said that in the early stages of silicosis, it is subradiological—that is, the damage to the lungs may not be easily visible on a chest X-ray or CT scan, but the lungs have already become damaged and vulnerable to tuberculosis. When silicosis patients are put on tuberculosis drugs, they slowly become vulnerable to the more lethal multidrug-resistant tuberculosis, or MDR-TB. Sarkar and three other researchers recently wrote a paper on this phenomenon, based on a study among glass-bangle workers in Uttar Pradesh’s Firozabad district. The glass bangles of Firozabad are renowned in India, but less is known about the workers who produce these bangles, many of whom have contracted silicosis as a result of their jobs, and have then contracted MDR-TB.
The paper’s findings were shocking. The study examined 402 glass-factory workers who had been exposed to silica dust regularly, of whom 186 were confirmed to have silicosis via radiography. The remaining 216 had been also exposed to silica dust regularly and, while their scans did not yet show it, were suspected to be in the early stages of silicosis. Of the confirmed 186 silicosis cases, 118 were found to also have tuberculosis. Meanwhile, the rate of tuberculosis among workers in the early stages of silicosis was far lower: 60 out of 216. The study compared these rates to a control group to conclude that as silicosis advanced, so did the rates of tuberculosis. The rates of MDR-TB showed similar outcomes: 16.4 percent of the confirmed silicotic workers, and 6.7 percent of the suspected ones. Five of the surveyed workers, who had silicosis and MDR-TB, died owing to the lack of proper treatment, the paper said. It termed silico-tuberculosis a “silent epidemic.”
“The decreased lung immunity in individuals with silicosis makes them more susceptible to TB infection, and the immune system’s ability to fight the bacteria is compromised,” the paper stated. “Additionally, the conditions prevalent in workplaces with high silica dust exposure, such as crowded living conditions and inadequate health care access, further contribute to the risk of TB transmission.” The spaces where silicosis is prevalent also happen to be places that lack the facilities and expertise required to diagnose and manage MDR-TB. “This delay in diagnosis and treatment initiation can contribute to the worsening of both conditions,” it added.

“When TB occurs with underlying silicosis, four things occur: difficulty in diagnosis, uncertainty of TB treatment, more chance [of] MDR-TB and more deaths due to treatment failure,” Sarkar told me. “When a person is treated for MDR-TB, it is more costly, [it has] more adverse effects, it spreads MDR-TB to family members, fellow workers, neighbours et cetera.”
Daya Ram Ahirwar, a 37-year-old from Gandhi Gram village in Madhya Pradesh, stood as testament to Sarkar’s point. Ahirwar had fallen sick in his late twenties and had been diagnosed with tuberculosis. His latest medical documents, which I saw when I met him in August 2023, said that he had developed MDR-TB. Ahirwar had worked for many years in stone mines and quarries. I showed his documents, including chest X-rays, to both Sarkar and Dutta. They both said that he had silico-tuberculosis. Their assessment was that Ahirwar likely had silicosis but had never been diagnosed with it. It is hard to say whether Ahirwar contracted tuberculosis because of his silicosis condition—and that is the tragedy, because both could have been prevented.
Sarkar emphasised the importance of early detection of silicosis. “There is an urgent need for the initiation of a national silicosis control programme, and TB elimination needs to be integrated with it,” he said. His list of suggestions was long. “The ministries of labour, health, mines, and industries all need to discuss together to develop a collaborative dual control mechanism for silicosis and silico-tuberculosis. Suitable legislation is required to be made for periodic screening and protection of all the silica dust-exposed vulnerable workers in the concerned workplaces of the country. National as well as state-wise silicosis registries to be maintained and digitised, which need to be linked with unique identifiers to track the silicotic workers longitudinally as many of the workers are migrant workers with frequent movement to other states.” The lack of data on silicosis, he noted, is a major impediment. “A deviation in lakhs can be seen in the TB data in India. So neither is the data of TB accurate, nor the data of silicosis. This is due to a weak and shallow system.”

How far the government is from implementing Sarkar’s recommendations is visible in its reports on tuberculosis. An official report on tuberculosis issued by the ministry of health and family welfare in 2023, which gives an update of the nationwide effort to eliminate the disease, includes only two mentions of silicosis in close to three hundred pages. One is to note that the government aims to increase tuberculosis-preventive measures among “priority populations such as diabetics, people using tobacco, people having silicosis etc.” The other was to note that the government’s tuberculosis-preventive module had an option for registering silicosis patients among those at high risk of contracting tuberculosis. There is no data on silicosis given in the entire report.
IV
SOME SILICOSIS VICTIMS I MET had been forced to turn activists in their own cause. Goaldaha is a Muslim-dominated village located in Minakhan block, in West Bengal’s North 24 Paraganas district. The Minakhan region is locally known for two reasons: poverty and silicosis.
Ramjan Paik, a Goaldaha resident in his late fifties, had buried his two sons. The family was struggling financially, and, like others in the village, his two sons had gone to work in the ramming-mass factories located near the border between Jharkhand and West Bengal. They were in their early twenties. They returned home within a few years, sick with silicosis, and died before turning thirty. “I have seen my sons struggling for every breath,” Paik told me. “What could be more painful than that for a father?” After their death, he offered a small home to local activists, to set up a makeshift health centre in his home for silicosis victims, with a bed and some oxygen cylinders. He said he did not want anyone else to suffer the fate of his sons.
West Bengal has seen people’s movements against silicosis, and the residents of Minakhan are aware of the disease, although they have few other options for employment. In 2018, the residents told me, villagers from around thirty villages across nine blocks of North and South 24 Parganas came together and formed the Silicosis Akranto Sangrami Shramik Committee, a volunteer group aimed at helping silicosis victims.
Aijul Paik, a silicosis patient who also volunteered for the SASSC, told me that the villagers of Goaldaha donated ten rupees a month to buy oxygen cylinders and beds for the health centre. Aijul had been diagnosed officially as a victim of silicosis, and received a card that made him eligible for government healthcare. Not everyone in the village had this option. “At midnight, when all of a sudden some silicosis victim needs oxygen support—to see their situation at that time, without oxygen, is very painful,” Aijul told me. “We have set up the centre to help those people die in less pain.”

The SASSC had gathered some data on the prevalence of silicosis in the region and found that more than seven hundred workers from the two districts had gone to work in stone industries and were at risk for silicosis. More than fifty workers had died of silicosis-like symptoms, but only 18 families had received a one-time compensation. According to SASSC, 39 living victims had received a silicosis identity card, of whom 31 were from Goaldaha. Through the efforts of trade unions and activist networks such as the SASSC, the state government was involved in testing over three hundred and fifty possible silicosis cases in two districts. Almost all of them had been working in quartz-grinding factories.
In Jhabua, I met a series of workers from various districts of Madhya Pradesh, who had migrated with their families to Godhra and Balasinor, in Gujarat, to work in the quartz-grinding factories. These workers were directly exposed to massive amounts of silica dust while filling bags, loading tractors and collecting stone dust. Even the areas near the factories, where they resided with their families, were shrouded in clouds of silica dust. The round-the-clock exposure resulted in many of them, even the family members who had not worked in the factories, falling sick and dying within a year or two.
Dinesh Raisingh, a 37-year-old from the Bhil community, had lost ten members of his family, including his wife and sister, to silicosis. His family members all worked in or resided near quartz-grinding factories. Raisingh hailed from Kachaldara village in Madhya Pradesh, and had wanted to break the cycle of poverty his family had been stuck in for generations. “We faced acute poverty here in the village—the situation was as good as starvation,” he told me. “We are compelled to go outside to earn our livelihood, and the nearest place from here is Gujarat.” In 2001, over thirty people from his village moved to Godhra to work. “We used to make powder from quartz, which is used to make glass,” he said.
“We were in financial crisis, so we opted to work for minimum rates at factories such as Dhartidhan and Hindustan,” Raisingh said. They earned 50 paise for a bag of stone powder, “so a group of twenty could earn a few hundred rupees a day, and one individual would earn at most fifty rupees a day. We somehow managed to survive on our earnings there, but at the cost of many lives.”


Raisingh had only worked at the factory on-and-off for a year but had fallen sick as well. “Our exposure to dust was so high that sometimes we would not be able to see the people sitting near us at the site.” The doctors he consulted in Godhra did not say it was silicosis, and he was officially diagnosed only several years later, in 2011. Now, he was at the stage where he was struggling to breathe and talk at the same time. He was worried for his daughter, who, as a young child, had stayed with him near the factories. “We are worried for those kids who were with their parents at the time,” he said. “Many have lost their parents, and others are alive, with silicosis. The serious issue is that even some children who were there have started facing breathing issues now, in their twenties.”
“My wife, my sister, my uncle’s four sons, and my sister’s four sons, all died there,” Raisingh told me. Now that villagers were aware of the disease, they avoided going to work in Godhra. He was worried that other poor people, from areas such as his, would still migrate, unaware what was in store for them. “Factories are still running, which means they have workers, which means silicosis is still there.”
Raisingh was now an activist in the Jhabua area, working with silicosis victims to have them officially recognised by the government and to seek compensation or relief. He was also one of the petitioners in a silicosis case being heard by the NHRC that eventually went to the Supreme Court.
ORGANISATIONS LIKE the SASSC and OSHAJ were active in nearly every state I visited. If there is a history of silicosis detection in India, much of it is thanks to these kinds of NGOs and activist collectives, which fill in the gap left by government inaction. Across various states, the documentation of silicosis—victims, occupational histories, patterns of migration—is maintained by such organisations. In some states, these groups played a central role in pressuring the government to formulate specific policies for silicosis victims.
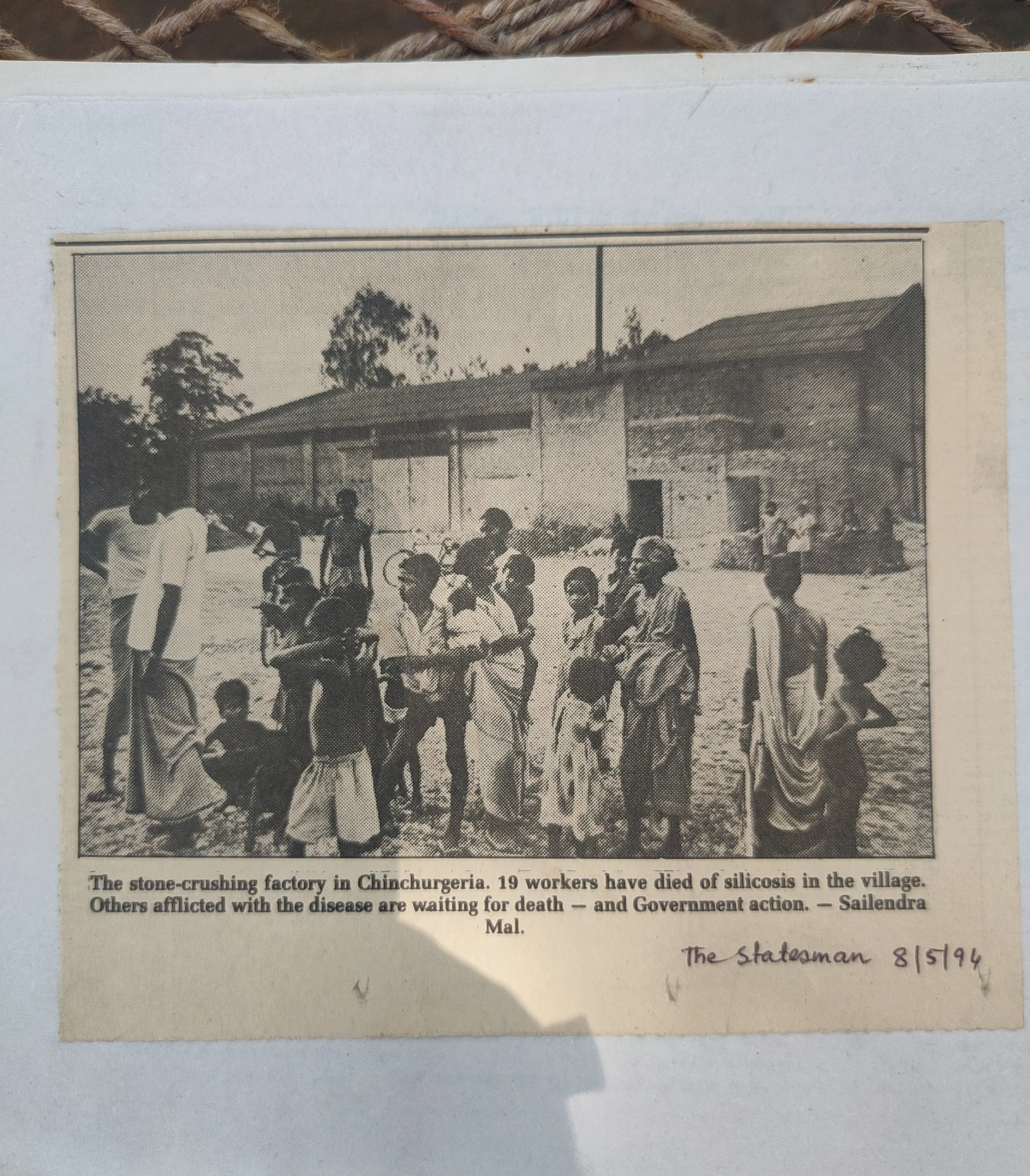
In West Bengal, silicosis was first documented officially in 1996, in Chinchurgeria village of West Midnapore district, when villagers staged an aggressive movement against factory owners in the area. I met Tota Santra, a health worker and activist in her late fifties, who has been tracking the movement since then. She had maintained a meticulous record of all media coverage of silicosis. Every news report on the issue, in Bangla, English and Hindi newspapers over the last thirty years, had been cut out and pasted into a scrapbook.
The story Santra recounted was familiar. Since the 1980s, the Adivasi residents of the village had been working at Surendra Khanij, a quartz-grinding factory in the area for ten rupees a day. “At that time, a layer of dust covered even the food and water,” Santra recalled. “It not only killed people but also damaged the forest as well.” Most workers quickly developed a series of health issues, such as silicosis, although most were told they had tuberculosis. According to Santra, 24 workers from the village died during the early 1990s.

In 1993, the Quark Science Centre, a local NGO, began testing the workers, and found they had silicosis. (One paper in the Economic and Political Weekly noted that they tested at least a hundred workers.) The workers had been protesting, demanding the closure of the factory. “Villagers told us that they had gathered twice at the gate of the factory, demanding its closure, but the police came and threatened them,” one activist told the EPW. “They became silent, in spite of fully knowing that the factory was the cause of their sufferings.” The local activists in the area began a wider campaign, including street meetings, protests and a signature campaign, eventually compelling the district administration to close Surendra Khanij.
Then, six central trade unions became involved and formed a wider platform, and filed a public-interest litigation in the Supreme Court, citing the impact of environmental pollution on workers’ health in West Bengal. The apex court directed the West Bengal Pollution Control Board to intervene, which, in turn, involved the local activists. The state government claimed that it had looked into the Surendra Khanij matter, that the factory was now closed and that, since the unit was not registered with the directorate of factories, no information could be gathered from either the management or the workers. The government also claimed to have found no cases of occupational illnesses in the local hospital. Eventually, the court directed the government to re-examine the matter, and it was forced to accept the truth of the state of affairs at Surendra Khanij—the WBPCB’s report admitted that the factory was operating illegally. It did not admit to a formal cause of death, but it said:
Out of the 20 deceased persons, 16 were found to have worked in the said crushing unit. No records relating to their deaths were available. Hence, their actual cause of death could not be ascertained. But from the verbal statements of the relations, it is revealed that all the deceased persons suffered from breathing troubles, weaknesses, etc. They were mostly engaged in jobs like sieving, bag filling with stone dust, loading and handling dust bags in a confined space, dust collecting.
In 1996, the court directed the factory to give compensation to the dead workers. It was to become a landmark judgment. “This was the first such type of case in which victims from Bengal got compensation or monetary relief,” Santra said. Though the activists had come up with a figure in the range of Rs 3 lakh, the government suggested Rs 50,000. The court eventually settled on Rs 1 lakh, admitting this was “on the lower side.” It directed the government to then rely on the Workmen’s Compensation Act to calculate compensation for the living workers who were suffering. The 1996 case did not lead to a statewide policy for compensation immediately, or even for many years. The poor residents of places such as Minakhan continued to migrate to nearby areas to work in stone-crushing years. The Telegraph reported that between 2012 and 2017, close to twenty people died in the villages of Goaldaha and Debitala, and that more than a hundred were ill with silicosis or severe lung diseases. Victims told the paper that doctors were not willing to sign death certificates stating silicosis as the cause of death.
This state of affairs continued for many years, even as activists and lawyers continued approaching the courts or the state authorities to take action. In 2018, the Calcutta High Court directed the state government to establish a silicosis rehabilitation policy. According to a local activist, in 2020, after massive demonstrations in the North and South 24 Parganas, the government released Rs 2 lakh each as a one-time compensation for 35 living victims of Minakhan, and also Rs 4 lakh each for the families of a few deceased victims. The broader policy was eventually put in place in 2022, and revised in 2023, after demonstrations by activists who felt it was not adequate. The state is now issuing identity cards to silicosis victims and aims to have screening centres in every district. As Dutta pointed out, this effort is only beginning, and the state only has two centres.
A robust policy would be life-changing for residents of remote villages such as Dhangikusum, in the Belpahari region, which are currently outside the scope of any government infrastructure or citizen initiatives. Chinu Sing, a 44-year-old Santal man who resides in Dhangikusum, has been suffering from silicosis for the past decade. The village is poor and isolated. Most villagers have no other means of getting around besides walking. And Chinu Sing cannot walk, because silicosis has eaten away his muscles and made him too weak. He had no money, no savings and no job. He lived in a one-room home, just passing his days, struggling to survive. His wife and child, too, had poor health, because they could not afford to eat even twice a day.
Chinu barely spoke when I met him at his village last year, with Jharna Acharya, a local activist. I gathered that he had visited a local doctor some years back but had never been officially diagnosed with silicosis, and had been taking tuberculosis drugs for three years. He had a history of working in mines and stone-grinding, and all the symptoms of silicosis. Kajal Sing, another resident who was sick, told me he had been working in mines since he was five years old. Both of them could not walk and were in no shape to access any health facilities.
I connected Chinu and Kajal to Dutta, who told me that Chinu’s old X-rays and chest plates showed signs of chronic cough, which could be due to silicosis or an infectious lung disease. He said that Chinu would soon require oxygen support to live. This was out of the question—unlike Minakhan, their village was remote and did not have any active civil-society organisations to help him.

We arranged for a car to come to the village and take them to a facility in Midnapore, about fifty kilometres away, where they got another scan. Looking at the latest scans, Dutta confirmed that Chinu had silico-TB and that Kajal had silicosis. An official diagnosis meant that they were now at least eligible for government compensation. If nothing else, it would help feed their families.
THOUGH RAJASTHAN has had a silicosis policy in place since 2019, the state is a window into how a lack of accountability plagues even the most progressive policies. States such as Rajasthan and Jharkhand, which have extensive mineral deposits of marble, granite, sandstone and clays—all with high silica content—are also centres of mining and home to the highest concentrations of silicosis victims. The mining industry contributes close to 4.4 percent of Rajasthan’s gross domestic product. The total number of silicosis patients in Rajasthan is unknown, but, according to a 2018 report by the comptroller and auditor general, about eight thousand silicosis patients were detected in the state between January 2015 and February 2017. Over the same two years, 449 people died of silicosis in just five districts. Regardless, the state still has no reliable figures for total silicosis patients, nor a database of active cases and their geographical spread. I heard multiple estimates from various civil-society organisations, but the figures were scattered, or specific to the regions where these organisations worked.
The Daang Vikas Sansthan is an NGO working in Rajasthan’s Karauli region, where Ramdev Jatav was based. According to the NGO, there are at least thirty victims in each of Karauli’s several hundred villages. The NGO had helped Ramdev and other victims like him access oxygen concentrators. Between February 2023 and May 2024, it provided concentrators to 58 victims in Karauli—although the need was higher.
Vikas Bharadwaj, the secretary of the Daang Vikas Sansthan, told me that, even though Rajasthan had been a mining hub for decades, silicosis was officially documented only in 2011. The NGO had been recording instances of lung disease among mine workers since it was founded, in 2008, and had identified around five hundred families whose cases it was tracking. All the families were extremely poor, and several patients had been told they had tuberculosis. The NGO found that 232 women were widows of men who had died from lung disease, and 116 people were bedridden with tuberculosis.
“We knew that those families were spending about sixty percent of their income on treatment of TB,” he told me. “Even though this is a curable disease, their TB was not getting cured even after taking a proper medicine course.” The NGO then decided to examine the cases of 18 families more closely, to understand why the tuberculosis treatments were failing. “Within six months, we found that no one got cured and five people died. We shared our finding with the government doctors and they said it was not TB but either silicosis or something else, but no one was ready to give the report in writing.”
Daang invited PK Sishodiya, the head of the National Institute for Miners’ Health, to visit Karauli in 2011. Sishodiya visited various patients and gave a written report that they did not, in fact, have tuberculosis. On the basis of this report, Bharadwaj convinced the district administration to conduct a radiography of over a hundred patients. He showed the radiograph results to a doctor at the government-run Jhalabad Medical College. According to Bharadwaj, though this doctor suspected silicosis, the college refused to give any diagnosis in writing. Finally, Bharadwaj visited Sishodiya in Pune and showed him the test results. “He saw all the radiographs and declared that 93 out of 101 showed silicosis, and hence silicosis officially came to the surface in Rajasthan.”
Devarajan was a member of the state’s human-rights commission, between 2011 and 2015, and was largely satisfied with the commission and the government’s efforts during this time. But even he acknowledged some core failures. He said that, beginning in 2013, the commission had taken an active role in taking a series of measures to deal with silicosis. “The attitude of the medical and medical education departments in Rajasthan has been reasonably positive,” he said. “But their main failure so far has been their inability to train the doctors in silicosis detection and treatment and not laying down standard operating procedures for these.”
The state government had established a pneumoconiosis board in 1967, but it was never functional, Devarajan told me. The commission intervened in 2013, and the government established such boards in seven medical colleges, to detect the disease. “The fact that so far they altogether have certified over forty-two thousand cases of silicosis indicates that they have managed to put their acts together,” Devarajan said. “However, there are several problems. The first one is lack of training and capacity-building, due to which there were several cases in which expert bodies like the National Institute of Miners Health, Nagpur, and AIIMS, Jodhpur, gave a positive diagnosis of silicosis, but the district boards gave negative diagnosis.” He likened this to “primary school teachers failing students in papers in which IIT and IIM professors gave them A+ grade.” Still, the government had been making efforts to sensitise doctors at the PHC and CHC levels, and he felt this would improve the situation.
Bhardwaj was a little less optimistic. “Hospitals are still missing the facility of pulmonary function test,” he said, referring to a test that reflects the strength of a patient’s lungs. The Rajasthan government had also launched a silicosis portal for workers to register themselves, but the portal required official documentation of employment, which was hard to come by for most informal workers.
The issue Bhardwaj raised is central to the silicosis problem in India, and repeated across the country. The working conditions of labourers in India, such as those working in factories and mines, are largely governed by labour laws such as the Factories Act, 1948, the Mines Act, 1952, and the Workmen’s Compensation Act, 1923, which mandate protection from exposure to dust and the provision of healthcare facilities, as well as compensation. These acts recognise silicosis as an occupational disease.
Some states have their own policies and laws, too—Rajasthan, for instance, being a mining-heavy state, implemented a mining policy in 2015 that recognises diseases such as silicosis and mandates that factories employ procedures such as wet drilling to reduce the dust or pollution workers are subjected to. Besides these, there are environmental laws and regulations that define the permissible limits for, say, air pollution at mines and factories. Workers are also eligible for social-security benefits under laws such as the Employee State Insurance Act, 1948.
But laws can only work in a formal system, where factories are officially registered with the government, and where they declare the number of workers they employ, and where workers hold proof of employment such as a contract and are registered with the government. This is not the reality for most of India’s industries. Most estimates, including recent government surveys, put the size of India’s informal economy at about eighty percent or more of its working populace. In the mining and quarrying sector, illegal units are par for the course and hugely underreported. Even registered mines or quarries rarely declare the full list of all their workers, hoping to avoid accountability. “Silicosis-affected workers in the informal sector are not entitled to statutory protection, which would remove them from the hazardous environment, or to compensation, which would enable them to leave work,” a 2016 paper in a WHO bulletin noted.

Rajasthan has over thirty thousand mine leases, but activists estimate the actual number of mines is several thousand higher. Rana Sengupta, a labour activist who has been working with mine workers for many years and heads the Mine Labour Protection Campaign Trust, said that around thirteen thousand unregulated factories were active in the Jodhpur region alone. The situation is similar in other regions of the state, such as Kota and Pindwara, and even across other states, such as Madhya Pradesh and Uttar Pradesh, where illegal mining has been documented widely. This means that most workers who were afflicted with silicosis during the course of their work were not covered under any law or government policy. Even those who were covered faced the uphill task of seeking government certification, and then compensation.
“Before the launch of the silicosis portal, there were more than ten thousand silicosis victims in Karauli alone,” Bhardwaj said. “Ironically, such labourers have no identity, no proof, that they are mine workers.” (In Jhabua, villagers had told me that, sometimes, workers who fell sick would run away without turning in their identity cards to their employers, because they were afraid that, otherwise, they would never be able to prove where they had worked.)
Sengupta pointed out that registration is challenging even for those with the necessary documents, noting instances of fake certifications issued by touts. While the government has digitised the certification process, the system often rejects genuine applications. “We frequently assist workers with the process, yet many face rejections,” he told me. “The system is neither smooth nor accessible for illiterate, unaware workers. There’s a pressing need for the system to reach out to these workers and conduct blanket tests to determine their silicosis status.”
The activists also noted that the compensation figures were still awfully low—both West Bengal and Rajasthan offer compensation that is only slightly higher than the figures that the Jhargram activists had devised in 1996. “Giving Rs 3 lakh under silicosis policy is nothing for them,” Sengupta said, “because they remain in crisis by repaying debt, taking more debt and suffering from the disease.”
Comparing the workers’ situation to bonded labour, Sengupta described how they are trapped in a vicious cycle of poverty and debt, often borrowing money from the very mine owners responsible for their illnesses. “Despite silicosis being recognised as an occupational disease qualifying workers for higher compensation under the Workmen’s Compensation Act, registration and proof of employment remain significant hurdles,” he said. “Labour enforcement in Rajasthan is a colossal failure, leaving those entitled to Rs 17 lakh or Rs 20 lakh with only Rs 3 lakh, which they often spend on medicines and repaying debt.”


Sengupta and Bharadwaj both noted that the focus of the government was only on detecting and giving compensation, but not on prevention—the only way to actually save lives. “Mine owners and the government are both responsible for the increasing number of cases,” he said. “The government must monitor the entire system, and the mine owners violating laws must be prosecuted.” He added that issues such as rehabilitation, alternative jobs, medicine and oxygen support, and access to doctors remain unaddressed.
A 2022 survey by the Sirohi district administration was a reality check to the Rajasthan government. The survey examined the Pindwara block, known for stone-carving, especially for temple stones. It was carried out by a team comprising several government officials from various departments and members of the Pathar Gadhai Mazdoor Suraksha Sangh, a stone-workers’ collective active in Pindwara, under the supervision of the district collector and the sub-district magistrate. Its findings clearly reflected the gaps the activists I spoke to had noted.
The report noted that the Pindwara block is among the most affected areas of Rajasthan. Almost half of the eight thousand stone-carving workers from Sirohi district who had been screened by the Rajasthan government had been certified by its pneumoconiosis board as silicosis victims. “High exposure of workers to Silica dust in these factories has caused large-scale poverty in the block, particularly among the highly vulnerable SC and ST communities of the area,” it said, referring to Scheduled Caste and Schedule Tribe groups. “The average age of Silicosis certified persons in the bock is in early thirties, causing high levels of mortality particularly among young men. Therefore, it is urgent to find a way to safeguard these worker-artisans’ lives, such that the art and livelihood of stone-carving can also be preserved. This underscores the urgency and importance of implementing the regulatory and preventive provisions of Rajasthan government’s Pneumoconiosis Policy.”
The survey team visited all stone-carving factories found in Pindwara block, both in urban and rural regions. It found 248 stone-carving factories, out of which it was able to conduct the survey in 230 factories. The report highlighted that there were huge gaps in the facts given by the factory owners and that there was a lack of safety and security measures. The dust particles at these sites were also found to be at a dangerous level. The report also highlighted that the ESI and provident-fund schemes were not applicable for most labourers, and that most of the labourers were working without any official record.
Only in seven cases were employers found to have provided health screenings to workers. Even in these cases, the health camps covered general ailments such as headaches and stomach aches, and did not include a chest X-ray or any test of lung function.

It is worth noting that Rajasthan and West Bengal were, in fact, states with better policies than most. In Uttar Pradesh, for instance, silicosis is yet to be officially recognised. GD Verma, a silicosis expert and activist from the state, said that government doctors were unaware of the disease and were not trained to diagnose it. He said that his organisation, the Bundelkhand Jeevika Sangathan, which had been working in the Lalitpur area of the state since 2009, had organised several camps to screen and identify victims, but the government had not acted on its findings. Like Rajasthan, Madhya Pradesh and Jharkhand have silicosis-compensation policies, but the activists and victims I met there reported the same problems: difficulty getting certified, lack of widespread screening, a general lack of awareness among both medical professionals and the victims themselves, and, most of all, a lack of any focus on prevention.
Amulya Nidhi, an activist who has worked extensively to document silicosis in Madhya Pradesh, echoed the need for meaningful government support. His organisation, the Silicosis Peedhit Sangh, surveyed 105 villages in Dhar, Jhabua and Alirajpur districts, and found 1881 cases of silicosis. The NGO estimated that 589 people had died from the disease between 2005 and 2016, of which nearly half were women. “As an NGO or organisation we have limited resources,” he said. “Whenever we reach a new area, we get new cases of silicosis. It shows the number is increasing, and that it is vast and beyond our reach to identify cases across all the districts and villages. It is the duty of the government to do so.” He, too, emphasised that without regulating factories, it would be impossible to curb the disease. Nidhi said the government was “insensitive” on the subject. “Is it possible for all labourers to reach the Supreme Court or the NHRC to fight for their rights?”
I sent queries to various state governments and relevant departments, seeking their responses on the findings in their states, their silicosis policies, as well as the silicosis data available with them. I attempted to call the chief secretaries of these states and relevant ministers. The administrative officers of the Uttar Pradesh, Madhya Pradesh and West Bengal governments had not responded by the time the article went to press.
Ajoy Kumar Singh, the principal health secretary of Jharkhand, told me that the government planned to roll out a digital portal with health data for the state, which would include silicosis data, and would be public. “On the subject of misdiagnosis of silicosis, we will take it into concern and do the needful,” he said. Kamal Singh Baghotia, the state programme officer for silicosis in Delhi, said that the silicosis policy was ready but yet to be notified. It was pending with the revenue department. He said that rehabilitation funds had been given in some cases, by the revenue department and the labour department, for workers in the organised sector.
V
A FEW DAYS BEFORE the inauguration of the Ram temple in Ayodhya, I met Prakash Meghwal, a silicosis victim, in Pindwara. The 44-year-old had played a role in the grand event: He had worked on the carved sandstone being used in the temple. Meghwal had even worked on some stones that were sent to Delhi for the new parliament building, he told me.

On the eve of the Ram temple inauguration, Pindwara was decorated in saffron in celebration. But Meghwal was consumed with anger and sadness. “My situation is critical and, for the last one year, I am on oxygen support,” he told me. “At this stage of life, breathing is the most difficult work for me. Sometimes, I don’t sleep the whole night because of breathing issues.” Meghwal was upset because, whenever he and other stone-carvers raised their voices against the impact of their work on their health, they were called “anti-Hindu” for opposing temple work.
Meghwal told me that no government, nor the owners of the factory he worked in, had helped him out. “The celebration of the Ram Mandir has another side, and that is not beautiful, but ugly, which is people like us dying in pain,” Meghwal said. “Look at us, not the temples.” He implored the authorities, such as the state and factory owners, to take some action and prevent workers from falling sick. “The government, the factory owners, all have some responsibility,” he said. “We will die, but at least save those who are not yet affected.”
Indeed, the most common concern activists and experts raised was the indifference of various governments, particularly the union government, towards silicosis. The NHRC is the only national-level body that has examined silicosis at any length. It intervened in 2003, when SA Azad, the president of the NGO People’s Rights and Social Research Centre, or PRASAR, submitted a petition before the commission. It detailed how the NGO had conducted a survey in the Lal Kuan village in the outskirts of Delhi, two years earlier.
The village was home to many stone-crushers, quarry workers, miners and construction workers who had lung diseases and who were not responding to tuberculosis treatments. Azad requested remedy on the grounds that the state government and contractors were neglecting the working conditions that eventually harmed the labourers. He also asked for a compensation grant for the victims. Many of the activists I spoke to, including Carr, had also approached the NHRC with complaints of cases from their states. Sengupta and Devarajan, too, had been involved in advising the NHRC.
For the next fifteen years, the NHRC drew attention to the disease by writing to the state governments, the union government and also parliament. In the early 2000s, the commission took cognisance of the various silicosis cases that had come before it and sent notices to respective state governments directing them to ensure rehabilitation and compensation. It noted the callous approach adopted by the governments, especially at the state level, towards the disease. During the course of a national review meeting on health, convened in March 2007, the NHRC categorically pointed out that silicosis is an occupational hazard. It emphasised the need for necessary intervention from the government and for involving ministries such as industry, labour and health, as well as the National Institute of Miners Health. It also constituted a national taskforce on silicosis, which emphasised that state governments had to take responsibility for acting on the issue and that union ministries should follow up with these governments.
In May 2008, after hearing from various state governments, the NHRC “observed that the occupational hazard of silicosis is preventable if proper warning is given and the working conditions are properly regulated and monitored.” Once a worker became afflicted with the disease, the commission said, “it becomes a constitutional obligation on the part of the Government to take appropriate measures for providing the necessary health care and rehabilitating the victims. The welfare of workers, especially those in the unorganized sector, should be given priority.” The commission also asked the union and state governments to respond to a ten-point questionnaire about actions taken to prevent silicosis, to document it, to compensate victims, and to enforce the provisions of labour laws.
PRASAR, meanwhile, also filed a writ petition in the Supreme Court, which passed an interim order, in 2009, directing the NHRC to seek any necessary assistance from the union health and labour ministries. It also stated that the NHRC could take up “specific and confirmed cases” of persons suffering from silicosis and recommend action.
The commission took several steps over the coming years. In 2010, it sent a list of 44 silicosis victims from Lal Kuan to the Delhi government, asking for details on what actions it had taken in these cases. That year, it also submitted a special report to the home ministry, to be forwarded to parliament, to “bring to light the pathetic conditions of labour involved in certain occupations which are at risk of this fatal disease.” In 2014, it organised a one-day conference to understand the action taken by the states and by the union labour ministry. Later that year, it also organised a meeting of silicosis experts to discuss action taken on the report that was sent to parliament.
The NHRC’s multiple notices and pleas fell on deaf ears. “The states seemed not responsive and, except a few, most could not give even a proper status report of silicosis. Unfortunately, till now, except in a few endemic states, there is no proper status report of silicosis and those reports too do not have much actual data,” Devarajan, who had been in several NHRC meetings, told me. “It is ironic that the exact data of silicosis is available neither at state level nor at central level.” Jagdish Patel, an activist from Gujarat, said that “the review meetings were never taken seriously, and that is why the subject is still caught in uncertainties.” Azad told me that even the concerned ministries seemed uninterested in acting on the NHRC’s directions.

The annual reports of the NHRC, too, mentioned the unresponsive approach of the states. One report said that, “in view of the non-responsive and insensitive attitude displayed by most of the States to the life threatening problem of Silicosis,” the commission had filed an application to be included in PRASAR’s case in the Supreme Court, which was still ongoing. As part of its application, the NHRC submitted recommendations on prevention, remedy, rehabilitation and compensation for silicosis victims.
Devarajan told me that the NHRC, too, eventually became inactive. “For quite a long time, until around 2017, things went well from the side of NHRC,” he said. “But, since 2017, it seems that silicosis is not their priority. Nowadays, one hardly reads or hears anything NHRC has done regarding silicosis.”
The union government, meanwhile, had been as good as missing in action. The NHRC had put much of the responsibility on the states themselves, almost relieving the union government of its responsibilities. Though the union government had tabled the NHRC’s special report with an “action taken” report, Devarajan said that this was not done until many years later. Hardly any action was actually taken on the recommendations, he said. “Nothing happened, and I am sure nothing will be happening in the future except in a few states, except the four states that have brought out silicosis policies,” he said. “Silicosis is bound to be there everywhere, so all states must take action to detect and prevent it, but most states are not serious about it.”
One major issue that prevents a true reckoning with silicosis is the absence of any real, reliable data across different government departments and bodies. In 2022, a member of parliament sent queries to the health ministry on the status of silicosis in the country and the measures taken to prevent it. The government’s failure to capture data became evident from its response. The health ministry responded that, based on the information from the labour ministry, the Directorate General Factory Advice Service & Labour Institutes has intimated 240 cases in Haryana during 2019; 34 cases in Haryana and 10 cases in Gujarat during 2020. No case was reported in 2019 and 2020 in Rajasthan and Uttar Pradesh. As per Directorate General of Mines Safety (DGMS), only 4 cases of silicosis in Andhra Pradesh and 2 cases in Kerala were reported in the country during 2021.
In 2021, the health ministry had said that in the ten years preceding 2018, Gujarat had seen 17 deaths due to silicosis, but that no cases of death had been found in Rajasthan and Jharkhand.
These figures are not only immensely low, but also do not agree with other data. I had met several patients in Rajasthan who had been certified by the government in 2019 and 2020, for instance, even though the union health ministry said there were no cases in this time. The government’s data on silicosis detection in Rajasthan between 2008 and 2018, too, did not hold up. According to a 2014 special report by the Rajasthan human-rights commission, it had detected 891 cases of silicosis and 57 deaths in just the previous two years. Jagdish Patel, the activist from Gujarat, too found the Lok Sabha numbers incorrect. “As per our records, we came across 13 silicosis deaths in Surendranagar, Morbi and Rajkot districts in 2019,” he told me. He noted that the government and DGFASLI numbers would only reflect registered factories. “So workers like the agate polishers in Khambhat or the stone-carving workers in Dhrangadhra will not be taken note of by anyone, anywhere, if they contract or die of silicosis,” he said.
I asked Devarajan to respond to the zero figure given for Rajasthan. “What do you want me to say on this, looking at the large number of mines, stone carving, cement industries, quartz grinding, sandstone and idol making and temple making involving thousands of workers?” he asked me. He said that he had been part of various meetings involving officers from the union government where the high incidences of silicosis in Rajasthan had been mentioned. “If, in spite of all this, the curiosity of none of these officers was raised about why they are not getting mandatory reports about the detection of silicosis, there is some serious lapse in the manner these officers and their offices function.”
I had written to the health and labour ministries to seek their inputs on a national plan for a silicosis policy, and on the data they had, among other queries. At the time of publication, I had not received a response.
Over the years, multiple silicosis-related petitions had been clubbed with the PRASAR case, and the apex court heard them all together. On 6 August 2024, the Supreme Court issued its judgment. It ordered the National Green Tribunal, the topmost forum for environmental issues, to monitor and oversee the impact of silicosis-prone industries nationwide. It also tasked the NHRC with overseeing compensation efforts.

Sanjay Parikh, a senior advocate at the Supreme Court, who once represented the NHRC in the silicosis case, expressed his dismay at the decision of the Supreme Court. He said the problem is increasing daily and would not be adequately addressed by remanding this serious issue to the NHRC and the NGT. “A holistic understanding of the problem of silicosis requires both preventive and remedial action. For that, the people who are suffering from silicosis need to be identified and given proper medical treatment besides compensating and rehabilitating the families of those who died,” he wrote to me over email.
Parikh added that each worker at every silicosis-prone workplace should be monitored and that every statutory body at every level needed to be tasked with ensuring that preventive measures were taken at every at-risk workplace. “Similar steps were required by all concerned, including the states and statutory authorities, to take preventative steps to minimise the impact of silicosis, including the imposition of strict emission standards.” The NHRC had given wholesome suggestions to the Supreme Court, he said, but these appeared to have not been considered. “Unfortunately, after 18 years of struggle and hope that the Supreme Court will resolve it in the interest of the lives and health of workers, including those working in the unorganised sector, the situation has come back to square one.”