Vietnam has less than 30 percent of the funding needed to fight tuberculosis. With only the most...






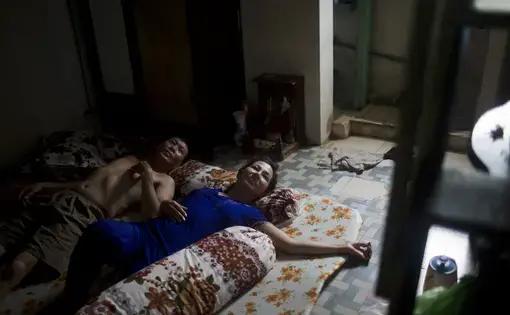
On a recent morning in a Ho Chi Minh City intensive-care unit, Cao Thi My Hanh sat crying and clutching her 5-month-old granddaughter, Nguyen Dang Thanh Phuong. More than a month earlier she had noticed the baby coughing and struggling to breathe. Hanh took her granddaughter to see several doctors in her rural province, but they all failed to give her a proper diagnosis. When she finally reached this large urban hospital, she found out that Phuong had tuberculosis, and realized the weeks of inadequate care had given the life-threatening illness time to take hold.
"I kept waiting and saw her coughing and turning pale," Hanh said over the din of crying babies. "If I had known that she had the disease, she could have taken the right medicines."
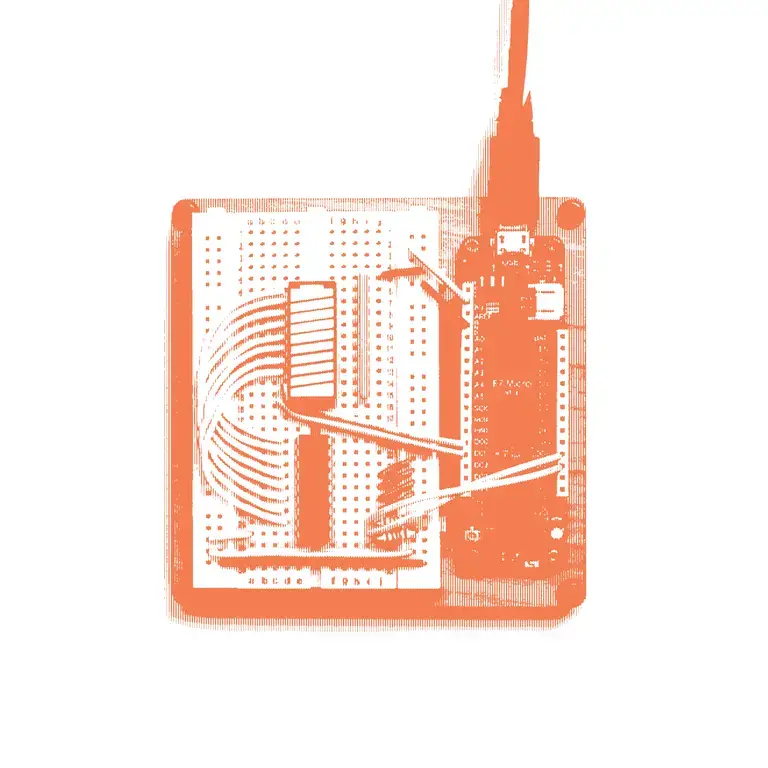
In a quiet laboratory on the grounds of this very hospital sat several gray and black machines that could have given Hanh a diagnosis much sooner. Hailed as the most significant advance in TB research in decades, this automated molecular technology called GeneXpert is more accurate and yields much faster results than traditional diagnosis methods, like smear microscopy, a basic test invented a century ago. To operate the machine, health workers deposit sputum samples they've collected from patients into cartridges that are then inserted into the Xpert machine, which is connected to a computer. The machine is able to detect the DNA of tuberculosis bacteria within 90 minutes to two hours.
When the California-based diagnostics company Cepheid Inc unveiled GeneXpert in 2010, the World Health Organization quickly endorsed it and global donors opened their purses to distribute it throughout the world. The result has been lifesaving for many patients, especially since the machine can identify multidrug-resistant forms of TB. Most recently, an Indian study published last month found that using the Xpert test increased the number of bacteriologically confirmed cases by 39 percent.
The problem is that not everyone has access to it. Not long after the rollout, health care workers began realizing that GeneXpert wasn't designed for the people who needed it most: the poor in the developing world. Even though donors were mostly paying for the $17,000 machines, the $10 cartridges were too pricey for many countries to afford on a mass scale. The setup also required electricity, computer access and refrigeration — not easy to come by in rural areas where TB is prevalent. As a result, the machines were underutilized in many hospitals and weren't being distributed to rural areas like Hahn's. In the Ho Chi Minh City hospital, for example, a mere 0.1 percent of TB diagnoses in 2013 were made with GeneXpert machines.
Ironically, though, those very limitations have ignited a sea change in tuberculosis care. The overwhelming excitement about GeneXpert among health officials and the substantial investments made by donors quelled doubts that there was demand for new TB technology and that it could be profitable. As a result, more companies have entered the TB market and are competing to develop diagnostic technologies that would provide the benefits of GeneXpert, without the drawbacks. The lesson? Often, it's the drawbacks, even more than the benefits, which can spur a paradigm shift.
Some context is important. Before GeneXpert, there hadn't been a major milestone in TB research for decades. Remarkably, most doctors were still using smear microscopy, which involves placing sputum samples on a slide and viewing them through a microscope. The technique is often ineffective because at times samples don't have enough TB bacteria in them to be detected visually. Because TB was largely regarded as unprofitable by the health care industry, research for new drugs was largely dormant, the development of new diagnostics tests was virtually nonexistent and the prevailing vaccine, invented in the 1920s, was proved to be largely ineffective for adults. All the while, TB remained the second-deadliest infectious disease in the world. Most troubling, millions didn't have access to adequate testing, and still don't. According to the World Health Organization, some three million cases of TB — one-third of the global total — still go undiagnosed.
"The word on the street was that TB was a disease of the poor and there wasn't enough money in it," says Dr. Madhukar Pai, director of the global health program at McGill University in Montreal.
But now, there are 81 manufacturers currently testing out 191 potential new products in TB diagnostics, according to a 2014 report by the global health organization Unitaid. Importantly, 11 of them are molecular technologies similar to GeneXpert.
"Because GeneXpert was a pioneer and showed the world we don't have to stay with this 100-year-old microscopy, that got the attention of a lot of companies," says Jim Gallarda, senior program officer at the Bill & Melinda Gates Foundation. "There is a lot of innovation now."
The Massachusetts-based diagnostics company Alere Inc., for instance, is using a $21.6 million grant from the Gates Foundation to develop a portable test that would be battery-powered, allowing it to be mobile for an entire day. The so-called point-of-care test would enable health workers to give a diagnosis to patients in the same place where they're receiving care, allowing them to make decisions about treatment on the spot. That would give it more reach than GeneXpert, which needs the electricity and air-conditioning of a health clinic to function. It would also cut down on the number of patients who never receive their test results.
"This is true point of care," says Duncan Blair, director of health initiatives at Alere. "I don't want to detract from Cepheid, but that's a lab system that requires refrigeration and power."
Alere is also working with Gates to make its machine and cartridges more affordable than GeneXpert's, and its increased mobility should help to reduce costs, too, Blair says. Alere is making the machine simpler to operate than GeneXpert as well, so that health workers don't need complex training. Finally, the Alere technology includes an efficient system of data collection and storage that sends results over a cellphone network to a cloud-based server. GeneXpert, on the other hand, requires a separate computer to store data, which has raised security concerns in poor neighborhoods. Alere plans to begin conducting trials on its product in 2016.
There are more technologies that could soon hit the market. The British biotech firm Epistem received certification allowing its Genedrive test, which can produce a diagnosis in 45 minutes and costs only around $4,000 per machine, to be marketed in the European Union. The Indian company Molbio Diagnostics' TrueLab technology can yield results in an hour, is battery-powered and costs only $6,000. The Chinese company Ustar received approval from its country's regulators to market its EasyNAT machine, while the British company QuantuMDx has received a grant from the Swiss-based nonprofit FIND to develop a similar test called Q-POC.
GeneXpert's limitations have also motivated Cepheid itself to make improvements. In 2012, Unitaid approved funding to reduce the price of the cartridges to $10 apiece from $17. Cepheid has also developed software called RemoteXpert, which uses cloud storage for data about TB patients. In a pilot phase in South Africa and India, the technology has allowed health workers access to real-time information from a database of nearly 2.5 million TB cases. Last year, the company announced an effort with FIND to develop a new model called Xpert Ultra, which will increase the ability to diagnose TB and H.I.V.
Still, there are questions. Cepheid has yet to make its machine more mobile. The technologies from Alere and QuantuMDx haven't been subjected to trials in the field, while the others outlined haven't had wide enough distribution to truly test their effectiveness. Alere points to a similar test it has used for H.I.V. diagnosis in several African countries. That machine has proved durable, as health workers even transport it across Lake Victoria on canoes to reach patients who live on islands.
These are the sorts of portable technologies that Hanh wishes had existed in her community in Vietnam. They might have helped doctors catch her granddaughter's illness sooner. "She is still so young, and it hurts me to see the doctor operate on her," Hahn said. "I just pray the she can overcome this difficult time."