A rainstorm passes over Interstate 94 in Morton County, North Dakota, on May 25. Inclement weather and long travel distances to medical providers present serious access barriers for seniors here, many of whom are not able to drive or are uncomfortable driving in low-visibility conditions. Image by Tim Evans/NPR. United States, 2024.
Senior health care access across much of rural America is in a state of crisis.
Decades of agricultural industrialization and consolidation have eroded rural employment opportunities, leading to a steady exodus of younger residents to suburbs and cities in search of work.
As small towns have depopulated, aged, and lost their economic base, their medical infrastructure has contracted in kind.
Hospitals, clinics, dentists, nursing homes, pharmacies — they have all felt the pain of increasing financial pressures. Most facilities depend on Medicare’s razor-thin reimbursement rates and alarming numbers of them have been forced to shutter operations in recent years.
Part of:
Randy Anderson has his eyes examined by Dr. Andrew Rodenburg during an optometry appointment on May 22. Anderson has to drive over an hour to Bismarck, North Dakota, to seek specialty care a few times a week on average, despite living two blocks from his small town’s hospital and clinic. Image by Tim Evans/NPR. United States, 2024.
Providers that stay open deal with many staffing challenges, with both money and skilled workers in short supply. Residents who remain find themselves stuck in a growing number of medical deserts. While these dynamics affect all rural residents, seniors — with their more frequent and varied care needs — are hit particularly hard.
NPR reporter Juliana Kim and I traveled across the Great Plains of North and South Dakota in May to photograph and document this predicament.
Along the way, we heard from a cross-section of Americans, including residents of shrinking farming towns, medical providers, assisted living facility staff, caregivers and Indigenous citizens.
Demolished walls surround a bathtub at a recently shuttered nursing home in Armour, South Dakota, on May 29. The facility, which operated as the only nursing home in town for many years, closed after sustained staffing and financial pressures. Image by Tim Evans/fNPR. United States, 2024. Dr. William L. Bender screens a patient with flu-like symptoms at the Heart of America Medical Center in Rugby, North Dakota, on May 14. Increasing numbers of rural hospitals such as Heart of America have become dependent on temporary contract providers such as Bender to fill their ranks as they struggle to recruit long-term practitioners. While these providers can offer a high level of care, they are more expensive to employ and do not provide stable staffing. Image by Tim Evans/NPR. United States, 2024. Retired nurse practitioner Lynda Hoerauf, 86, is pictured at her home in Hebron, North Dakota, on May 23. Hoerauf, who tried to retire four times but was continuously asked to return due to staffing issues, worked at clinics in Hebron and surrounding communities for nearly five decades before she finally left. The clinic, dental office and chiropractor in Hebron have since closed down. Image by Tim Evans/NPR. United States, 2024.
"My husband had Parkinson’s. … We had been paying all those years for nursing home insurance. Well, he ended up in the nursing home for 24 hours, then he passed away. So we probably lost $50,000, you know? But what do you do? You’re damned if you do and damned if you don’t."
—Lynda Hoerauf, 86, Hebron, North Dakota
The Rev. Gary Benz offers Holy Communion to Viola Weinhardt, 94, at her home in Glen Ullin, North Dakota, on May 24. Benz offers Communion and the chance to connect with homebound, often socially isolated seniors who are dealing with health issues. Image by Tim Evans/NPR. United States, 2024. Kyla Sanders, the program coordinator with the western Morton County Aging in Community project, poses for a portrait at her office in Glen Ullin, North Dakota, on May 23. Sanders wears numerous hats in her role, which is aimed at connecting seniors in the medically underserved area of western Morton County with a variety of essential resources that improve their quality of life. Image by Tim Evans/NPR. United States, 2024.
"Some people will just say, ‘My daughter calls on Sundays. And that’s the highlight of my whole week. I get to talk to someone on Sundays, so I know that I can make it the next six days.’ That’s crushing loneliness and that’s something we need to address right away."
—Kyla Sanders, Glen Ullin, North Dakota
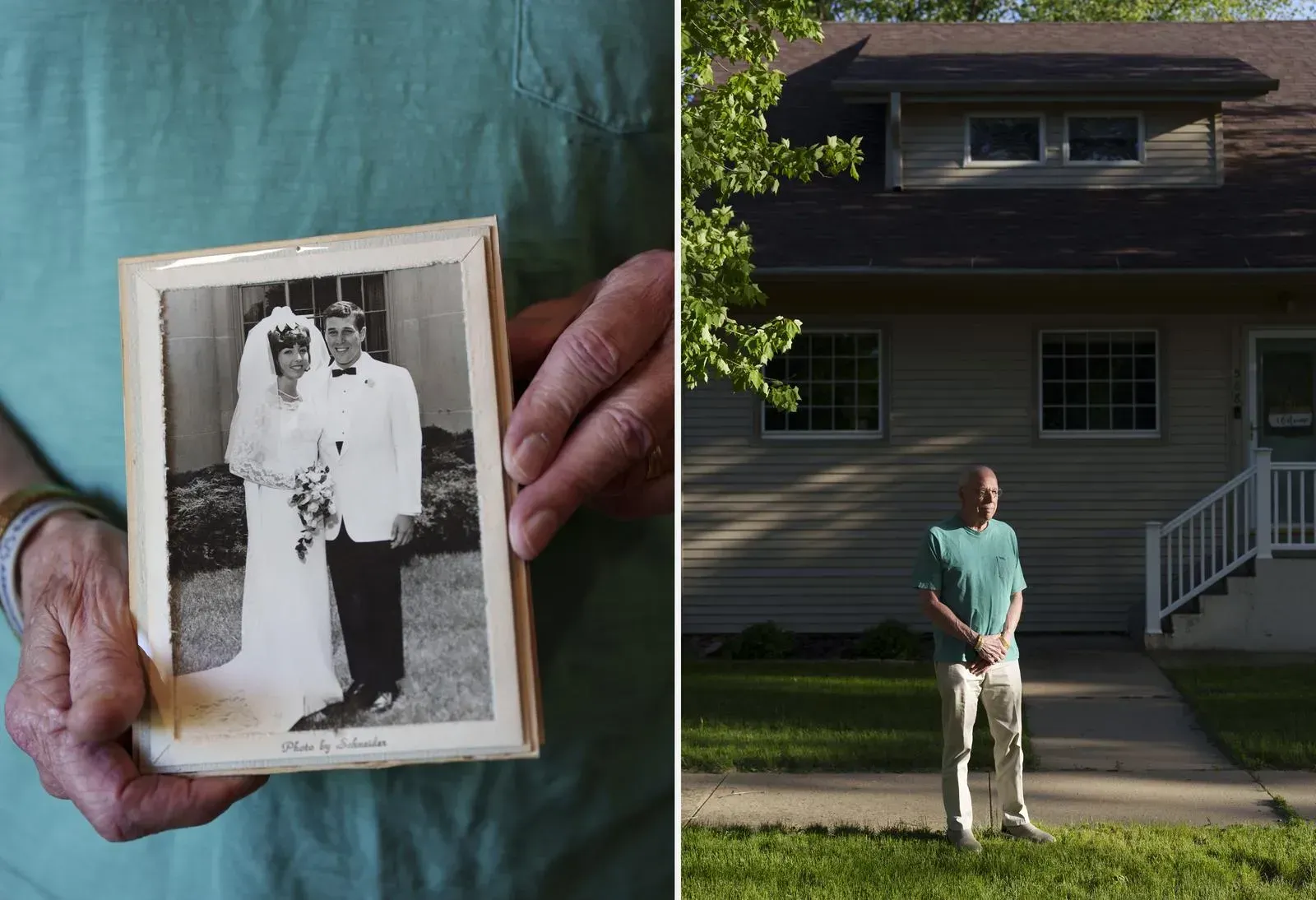
Tanya Urquieta, who was working as a project coordinator for the Older Adult Resource Network, would help connect seniors in the medically underserved areas in South Dakota's Douglas and Charles Mix counties to vital services aimed at improving their health and maintaining independence. Image by Tim Evans/NPR. United States, 2024. John Chicoine watched videos on YouTube for how to apply makeup and style hair for his wife, Paula, after she was diagnosed with Alzheimer’s. For five years before she died in 2023, he was her 24-7 caretaker. Chicoine stands in front of his previous family home in Parker, South Dakota, on May 18. After the Chicoines lived in the small town of Parker for over four decades, Paula’s worsening condition led the couple to begrudgingly relocate to Sioux Falls for medical support and housing to accommodate Paula’s needs. Image by Tim Evans/NPR. United States, 2024.
"If you’re a caregiver, you’ve got to be a doctor, a nurse, a dietician, an activity director."
—John Chicoine, Sioux Falls, South Dakota
A plane flies over the Beacom/Reischl Transitional Care Unit and Oakwood Assisted Living facility in Sioux Falls on May 18. Senior care facilities are in short supply across much of rural America, especially in depopulating areas of the Great Plains, where a majority of facilities are concentrated in larger cities. Image by Tim Evans/NPR. United States, 2024. Adolfo Pino, 73, prepares a batch of local newspapers for delivery during a work shift at Rocket Printing in Armour on May 29. Pino, a Cuban immigrant, is a participant in the Older Adult Resource Network, which connects people aged 65 and older in South Dakota’s Douglas and Charles Mix counties to resources to maintain their quality of life. Pino and his wife, Neri Jorge Cruz, have benefited in various ways from the program, including Spanish translation for medical appointments as well as financial assistance to help cover otherwise prohibitive health care bills. Image by Tim Evans/NPR. United States, 2024.
From having to drive hours for emergency or specialist care to dealing with a patchwork system of health insurance, older rural people confront a range of access struggles, with many left to ration or forgo care altogether.
We also learned about various attempts by committed providers, nonprofit organizations, state employees and community members to help close some of the many coverage gaps.
Carmen Magee prefers being close to her husband, Fred, who has Alzheimer’s, but it can be tough when she has medical appointments or errands to run. When Carmen traveled to Washington, D.C., for a few days to advocate for Alzheimer’s awareness, she needed 11 of her friends, family and neighbors to provide round-the-clock care for Fred. Image by Tim Evans/NPR. United States, 2024.
"People tell me, ‘Take care of yourself, caregivers need a break.’ But I ask: How do we make that happen? That’s why we need respite care, especially in rural places."
—Carmen Magee, Fort Pierre, South Dakota
A nurse checks a patient’s pulse following a cardiac stress test during a special monthly visit by a cardiology team to Douglas County Memorial Hospital in Armour on May 30. Image by Tim Evans/NPR. United States, 2024. Bryan Hochhalter and his dog Riley sit for a portrait at Hochhalter’s home in Bismarck on May 13. Hochhalter, a pastor, was diagnosed with Parkinson’s disease more than eight years ago and helps in a Parkinson’s support group in Bismarck, meeting with people who are newly diagnosed. Image by Tim Evans/NPR. United States, 2024.
"It’s just the nature of a state with some 750,000 people. And when you’re so spread out, specialists doesn’t tend to want to come here."
—Bryan Hochhalter, Bismarck, N.D.
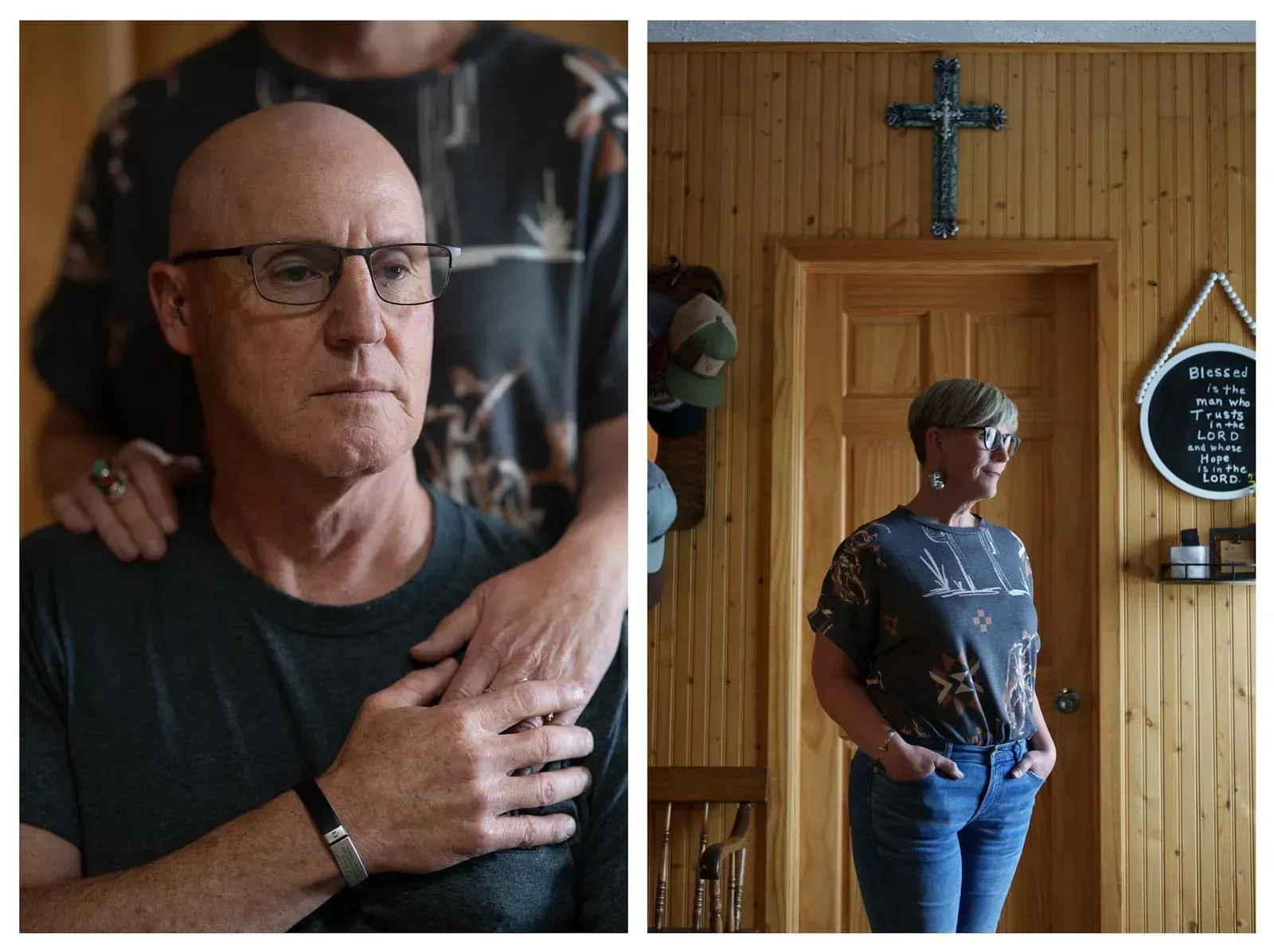
Wade Kottre, an EMT on the Glen Ullin Ambulance Service, stands for a portrait on a county road in Glen Ullin, North Dakota, on May 25. The ambulance service is staffed entirely by volunteers and provides an essential service for Glen Ullin and the surrounding area. While many of the volunteers are seniors themselves and have worked on EMT crews for decades, some younger volunteers have joined the team in recent years. Image by Tim Evans/NPR. United States, 2024. In Rugby, North Dakota, Jim Jundt and Tamra Kragness met when Jundt’s wife got sick last October. Kragness works for FirstLight Home Care. She helped the couple with chores and home-cooked meals. In March, Jundt’s wife died. Since then, Kragness has played an even bigger role in supporting Jundt, from taking out the garbage to driving him to his doctor’s appointments an hour away. But he can only afford about 11 hours of care per week. Jundt lost his leg a few years ago from an infection. Image by Tim Evans/NPR. United States, 2024.
"Tamra and FirstLight have been a lifesaver for me."
—Jim Jundt, Rugby, North Dakota
Dr. Richard Clark, a cardiologist from the Sanford Cardiovascular Institute, and a team of nurses spend a day each week traveling from their Sioux Falls offices to one of four rural hospitals that do not have cardiologists on staff. He checks a patient’s heartbeat during a monthly visit to Douglas County Memorial Hospital in Armour. Image by Tim Evans/NPR. United States, 2024. Louis DeCouteau, a member of the Standing Rock Sioux Tribe, is pictured at the Good Heart Community Center in Solen, North Dakota, on May 27. DeCouteau and other tribal members experience numerous health coverage gaps on the reservation. The Indian Health Service, a federal agency, tries to recruit health care workers by offering to help medical students pay off their loans in exchange for a two-year commitment to work in Native American communities. But DeCouteau wishes there were more full-time physicians around. Image by Tim Evans/NPR. United States, 2024.
"We have gotten good doctors in the past, but as soon as they get good, what happens? ‘Well, I paid off my loans, goodbye.’ Here comes another doctor to test us as lab rats."
—Louis DeCouteau, Solen, North Dakota
Randy Anderson flips through a calendar filled with medical appointments at his home in Turtle Lake, North Dakota, on May 22. Anderson and his wife, Marlys, who both deal with various health concerns, find their regular trips to Bismarck for care to be a considerable burden. “It’s like a full-time job almost,” Anderson said. Image by Tim Evans/NPR. United States, 2024.
 September 5, 2024
September 5, 2024