Project
Ending AIDS
An on-the-ground look at efforts in Africa and the United States to end the HIV/AIDS epidemic.











NYAMUTORA, Zimbabwe — For decades, this speck of a village was just like hundreds of others in this poor, badly governed, and HIV-ravaged country: Villagers watched as one person after another slowly withered from AIDS, rib cages jutting from torsos, cheeks sinking, and a hodgepodge of infections running riot through their organs. But now, Nyamutora is a model of how an innovative response to this disease can actually help end the AIDS epidemic across rural Africa.
A five-year-old program here has solved a surprisingly vexing piece of the HIV puzzle: making sure infected people take their drugs. HIV medications are extremely effective. If taken properly, they make the virus all but disappear from the bloodstream, which has two big effects. One is that it restores the immune system, allowing even very sick people to become healthy again. The other is that it almost eliminates the risk of spreading the virus. Keep the transmission rates low enough and the AIDS epidemic will die out altogether.
But this one-two punch only works if people can get the medications in the first place and then stick to their regimens. If they lapse, because of side effects or any other reason, the virus roars back, as does their chance of passing it to someone else. In the United States, studies estimate that only about 35% of people who know they're HIV-positive are on the medications and have virus levels so low they can be regarded as "undetectable."
In impoverished Nyamutora, it is 96%.
"This is incredibly good news that they have figured out how to sustain a lot of people on therapy with minimal resources," said David Katzenstein, an HIV/AIDS researcher from Stanford University in California who has worked in Zimbabwe for 30 years and leads the HIV testing of the villagers' blood.
Currently, fewer than half of the 37 million HIV-infected people in the world receive anti-HIV drugs. To break the back of the AIDS epidemic, the Joint United Nations Programme on HIV/AIDS (UNAIDS) has laid out an ambitious 90-90-90 goal: Over the next four years 90% of people should know their status, 90% of people who know they are HIV-positive should start on anti-HIV drugs, and 90% of those people should see the virus levels in their blood drop below the threshold where they can be detected. This week the U.N. General Assembly will meet in New York to galvanize political support for this program, but a major obstacle is money. UNAIDS estimates that achieving the 90-90-90 goal will cost $6 billion to $7 billion more each year.
So unless that cash materializes, the best hope is figuring out how to do more with less — and Nyamutora offers a powerful example of how this can happen. The heart of it is simplicity: Bring the drugs directly to the people who need them, and at the same visit conduct the crucial blood tests that tell whether they are working.
In the United States, lavishly funded research hospitals have multimillion-dollar machines that can reveal how the virus affects a dozen different types of immune cells. DNA sequencers spell out the genetic code of the virus and help doctors decide which drugs will work best for each individual patient. The higher-end clinics resemble art galleries, and nurses and doctors often have computer tablets that allow them to tap in patient information or retrieve case histories. Such shiny, high-tech, sophisticated systems can of course deliver state-of-the-art care, and they helped provide much of the research underpinning the three dozen antiretroviral drugs that have spared millions of people from dying horrible deaths from AIDS.
But when it comes to ending the epidemic, none of this is necessary. Just look at Nyamutora and ask a question that Zimbabweans rarely hear from outsiders: What, exactly, are you doing right?
At 7 a.m. on the warm, clear morning of November 27, doctors, nurses, pharmacists, and orderlies gathered in a rectangular courtyard of the Chidamoyo Christian Hospital, as they do at the start of each day, to sing. Shortly after the hymn, a Land Cruiser stuffed with anti-HIV drugs and five staff members took off for Nyamutora. They drove for 90 bone-rattling minutes over the rutted roads that crisscross this tobacco-farming region of Zimbabwe's Mashonaland West, and when they arrived, 150 villagers were waiting for them at the local church.
The adults were decked out in their Sunday best, with women in their finest dresses and splendid headwear, and men sporting slacks and collared, pressed shirts. But many of the children had on their school uniforms, because this was not a Sunday morning service. It was a Friday and there was no holiday, no wedding, no baby dedication. Today was an event that occurs every other month, and the attendees had dubbed it Chidamoyo Day.
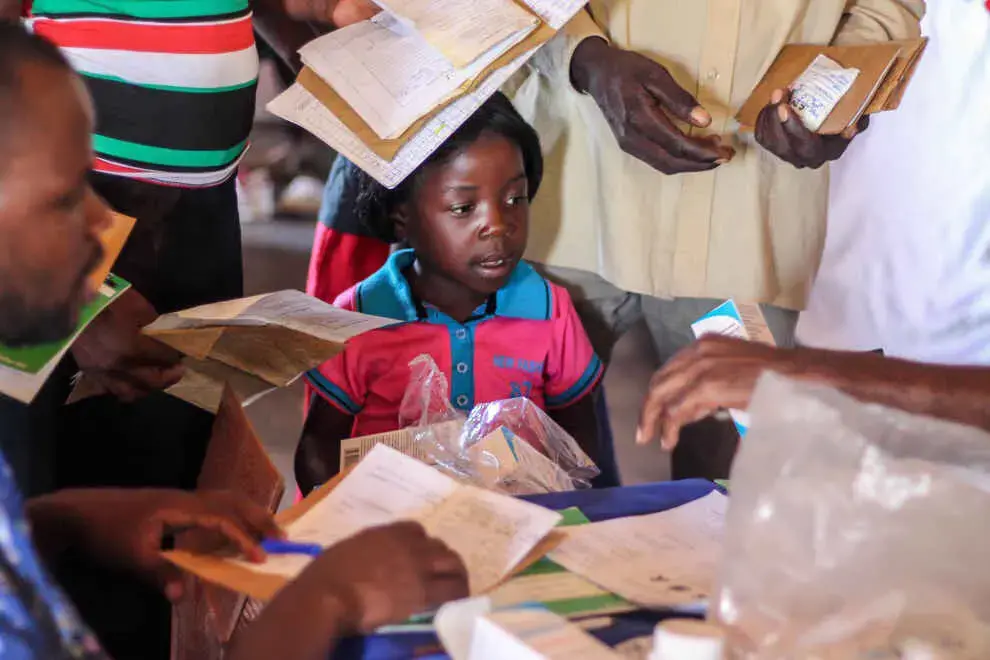
As the Chidamoyo team unloaded the boxes of drugs, medical records, and condoms from the Land Cruiser, the villagers rose from worn wooden benches to dance and sing a song of praise. Alvin Muparadziwa, a nurse from Chidamoyo, spoke to the group. "I'm happy about the levels of HIV in your blood," Muparadziwa told the gathering. "All your results are very good."
After the Chidamoyo team handed everyone their medical records, the adults and children queued up in separate lines to receive their two-month supplies of antiretroviral drugs and have their weights checked. Standing in line was the headman of Nyamutora, Matford Mtandazo, known to everyone as Sabuku, which means "the one who keeps the book" of the 56 community households.
In 2008, the older of Sabuku's two wives, Rumbidzai, had tested positive. Their story shows why HIV kept killing so many people here even after antiretroviral drugs became available — and why the new program has achieved such success.
At first, Rumbidzai believed she merely had malaria and only was given an HIV test the third time she sought care. "I was surprised and thought, Where could this come from?" she said. At the time of her diagnosis, Rumbidzai had lost 35 pounds and learned that her immune system had almost completely collapsed. HIV targets and destroys white blood cells, known as CD4s. On standard tests, healthy people have from 600 to 1,200 CD4s. Rumbidzai only had 164 CD4s, leaving her vulnerable to even wimpy infections.
For the first year after testing positive, Rumbidzai, who had seven children with Sabuku, lived with relatives in the city where she grew up, five hours by car from Nyamutora. She received antiretrovirals and a year later returned home, her immune system improving and her weight returning. But even though her husband saw how the drugs revitalized her, he didn't get tested himself. "I was feeling healthy," he shrugged.
He also admits that he was afraid of the stigma. People associated the virus with promiscuity, and they shunned the infected. "People would even refrain from eating with you because they'd think you'd contaminate them," he recalled. He and his wife kept her infection a secret, telling no one outside their family.
Meanwhile, she kept traveling back to her childhood home every two months to receive her pills. The trip soon became too expensive, and she switched to a clinic closer by, but transport still cost the equivalent of $5 each way, not a trivial sum for the family. Walking to the clinic would have taken the better part of a day.
By 2012, the virus had taken its toll on Sabuku and his second wife, Anna Chenjerai, mother of three more of his children. Both had lost many pounds. Sabuku, who ran a building contracting company, no longer could work. They had difficulty paying the school fees for their children and were driven to sell vegetables from their garden and even — in a sign of utter desperation — some of their livestock.
Finally, they got tested for HIV. Like 1 in every 6 adults in Zimbabwe, they were positive. Worse, they had almost no CD4s, the immune system's infantry. "I had 22 soldiers," said Sabuku. Anna had 14.
Chidamoyo Days had started in the village the year before. The idea came about because most villagers are Salvationists, and a nearby Salvation Army church had begun periodically sending a truck to Nyamutora to take the growing number of HIV-infected people to and from a clinic. Church representatives then approached the Chidamoyo Christian Hospital and offered to pay for gas if the hospital would send staff to the village instead. "We went through our records and realized a lot of our patients lived there," recalled Kathy McCarty, the nurse in charge at Chidamoyo. The cash-strapped, overwhelmed hospital — which, when the economy bottomed out a few years ago, actually accepted payment in peanuts — also saw that an outreach program could ease their patient load.
Around the same time Chidamoyo Days began, monitoring people had become simpler and cheaper. A newly developed portable machine allowed them to measure CD4 counts in the village. Katzenstein's group introduced a novel way to test how much HIV is in a person's blood. It requires only a finger prick and a drop of blood, which then is dripped onto a piece of paper that can be later tested in a laboratory.
"We are alive because of the Chidamoyo program," said Sabuku.
While the program has clearly helped Sabuku, he has also helped the program.
"It has a big effect that Sabuku and his wives come," says McCarty. "It's an encouragement to people." Sabuku has become a proselytizer for HIV treatment and reducing stigma, standing up at community meetings and pronouncing that he is as healthy as someone who is not infected. "I might as well tell the world I'm fine," said Sabuku. "I tell people once I was very sick and now I'm fit because I know my status."
The mass gathering of HIV-infected people further minimizes stigma and has everyone in everyone else's business — in a good way. "Politically, there's pressure for people to come and get their own drugs," said McCarty. And villagers who miss a Chidamoyo Day are identified then and there — and have to travel all the way to the hospital to get their drugs.
McCarty, who is from California and has worked at Chidamoyo since 1980, half jokes that the villagers rarely forget to take their meds because they are afraid of her. "I tell them, 'If you default, I'm not coming to your funeral, so you better take your drugs,'" she said. "And I tell them from the start that you can become resistant to these drugs very easily, and Zimbabwe has very limited second-line drugs, so if you become resistant I hope you can climb across the border to South Africa."
For many villagers who have had AIDS and recovered, one of the strongest motivations to show up on Chidamoyo Days and to take what they call their "tablets" without fail is the fear of their bodies withering again, becoming so weak that they cannot work in the fields or care for their children. As one of the villagers said, "I might forget to put on clothes, but I never forget to take my medicine."
This helps explain why children infected at birth now present one of the most perplexing challenges.
While the last adults inside the church received their boxes containing bottles of antiretrovirals, 13 kids, 7 to 19 years old, gathered under a tree outside of the church to meet with Nozipo Ncube, a middle-aged woman who is a counselor but looked like a queen in her shiny gold taffeta dress and matching headdress. "If you have any problems," she said, "you must not hesitate to ask me questions."
Health care workers the world over wring their hands about children infected at birth who often start shunning their pills when they reach their teens. Some began taking antiretrovirals before they could talk, and because they have never become ill from the virus, they don't see the point. Others went untreated and only learned of their infections when they developed AIDS themselves, at, say, 10 years of age, which can lead to a supercharged version of teen angst, confusion, and defiance. But perhaps the biggest problem is the very success of the drugs: Many teens in Nyamutora now see few people dying from AIDS.
Ncube's group counseling sessions aim to help these children understand the stakes and take their medication. "You're going to be taking these tablets most of your life, even if you don't have disease, even if you're married," she tells the group as a hen struts around the group with her chicks scrambling behind her. "It's not your fault that you got this virus: No one chose to get the disease."
Chidamoyo Christian Hospital now has similar projects underway at seven other villages. None has an HIV-infected headman who plays the influential role of Nyamutora's Sabuku, and none of the other villagers have had their HIV levels or CD4s monitored. But McCarty has no doubt the programs are saving lives. "The community gatherings encourage people to take their drugs and to be there every two months," says McCarty. "It's like a family. You want to go and meet your friends and see how they're doing. They'll say, 'Oh, that guy has improved so much.'"
She is certain this would work in many places around the world. "It's very exportable," says McCarty. "We don't do anything special at all."
There are limitations. Staging Chidamoyo Days might not make sense in cities, where myriad clinics provide care and social ties are looser. Still, about 70% of the HIV-infected people in the world live in sub-Saharan Africa, and millions of them make their homes in villages that do not have paved roads, are distant from clinics, share water pumps, and have one place of worship and one school for the kids. Same holds for hard-hit communities in Asia, which accounts for 13% of global infections.
UNAIDS's 90-90-90 goal aims to end the global AIDS epidemic by 2030. "The End" does not mean the virus will disappear from the human population — that's a feat only possible with a vaccine, which likely remains far off. But epidemics only keep rolling if, on average, each infected person transmits the virus to at least one other person. Over time, the decreasing number of people infecting others will cause the epidemic to peter out. The End also means preventing HIV-infected people from developing AIDS.
There's a most human variable that will arise even if the money is found to treat all 37 million people living with the virus today: What will motivate them to go on drugs and take them day after day, for decades? Nyamutora spotlights a simple, cheap, and effective way to help people to stick with it.