


Project
The Ebola Outbreak in North Kivu
What happens when Ebola hits in a war zone?

Tedros Adhanom Ghebreyesus concentrates on a map of a long-forsaken war zone in the northeastern provinces of the Democratic Republic of the Congo (DRC). Ebola is gaining ground here, and Tedros, the director-general of the World Health Organization (WHO), needs to stop it. He huddles in a dim corner of a mess hall with his officers on the front lines. Their fingers dance across the map as they point to areas occupied by militia, and explain how their teams struggle to circulate through these parts with vaccines and thermometers, key tools for limiting Ebola’s transmission.
As darkness falls, more WHO staff file into the hall at the United Nations compound in Butembo, a volatile city in North Kivu province. The din of their conversations rises as a buffet of stewed meat, fried fish and plantains gets cold and some boxed wine grows warm. Eventually, Tedros, as he prefers to be called, ends the meeting with his top aides and announces that it’s time to eat.
He settles into a chair at a table of young Ebola responders — mainly Congolese public-health specialists and physicians — and falls silent. It was June, and Tedros was facing pressure from all directions. The outbreak had already grown to be the second largest in history. And despite having a new Ebola vaccine and drugs to treat the disease, the death rate was soaring at 67% because the therapies weren’t reaching everyone in need. Armed groups weren’t the WHO’s only challenge. Many residents just didn’t accept that Ebola responders were there to help. A deep-seated scepticism of outsiders comes from more than a century of conflict, exploitation and political corruption in the region. And wars over the past 25 years have destroyed any semblance of a reliable, regulated health system. “The outbreak of Ebola is a symptom,” Tedros explains. “The root cause is political instability.”
This explanation doesn’t satisfy health-policy analysts who observe the escalating outbreak — which has killed more than 2,000 people — and question the WHO’s ability to contain it. Their criticism comes just as the organization is asking governments and philanthropists to give millions more dollars for the response. The WHO has more Ebola responders on the ground than any other international organization because ongoing violence keeps many others at bay. The responders have faced death threats and stones, bullets and grenades.
Tedros had come to Butembo to hear about obstacles, and to speak to leaders around the city about calming tensions so that his teams could work without harm. As he eats with the responders, he grows defensive on their behalf. “They are working day and night,” he says. “Other groups come and stay for a few hours; they run when they hear one bullet fired.” He rests a hand on the shoulder of an epidemiologist sitting beside him. Her colleague, Richard Mouzoko, was shot dead at a hospital in Butembo two months earlier. “She’s taking the same risk Richard took,” Tedros says. “We are doing this to save lives.”
Violence and Mistrust
In the morning, Tedros heads into the luminous forests on the outskirts of Butembo in a convoy of black armoured jeeps. In the town of Katwa, the vehicles pull over at an Ebola treatment centre that came under fire a few months earlier. Snipers from the DRC army now guard its entrance. Tedros strides rapidly through the wards and poses for a flurry of photographs with his team wearing WHO tactical vests. “I am very proud,” he tells the workers. “Even when I’m not around, I am thinking of you.”

In a flash, he is back in the motorcade, rushing to a runway where a helicopter awaits. Ibrahima Socé Fall, the official leading the WHO’s Ebola response on the ground, sees Tedros off. I stay behind with Fall, to see what it means to battle one of the most deadly pathogens known to humankind in a city tortured by war.
We slide into an armoured vehicle and head north to the city of Beni on an unpaved highway that slices through tall grass and lush, tropical trees. This strip of land is controlled by grass-roots militia groups known as the Mai-Mai, so the vehicle moves at a steady clip behind a pickup truck carrying soldiers in the back. When the sky opens with heavy rain, they pull faded winter parkas over their heads.
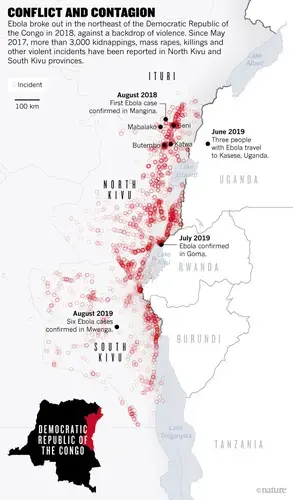
On the drive, Fall talks about the toll of violence. A surge of killings, arson and gang rapes has traumatized communities. Around 1,900 civilians have been massacred in North and South Kivu in the past three years and another 3,300 people have been abducted, according to the Congo research group, a non-profit investigative project at New York University (see ‘Conflict and contagion’). Parents mourn for children who have been stolen and forced to serve as soldiers. “The people here are very stressed,” Fall says. He notes that clashes a week earlier, in the Ebola-stricken province of Ituri, killed 160 people and sent 300,000 fleeing for their lives. It hardly made the news. “The people here don’t believe that anyone cares for them, even their own government, so it’s very hard to convince them that we are here to help,” he says.
The roots of mistrust run deep. The east has been embroiled in wars that began in 1996, after the genocide in Rwanda spilled into the DRC. At least eight other African countries were soon involved in what became known as Africa’s World War. By 2007, an estimated five million people had died from violence, disease and malnutrition as systems crumbled. Although the wars have technically ended, around 130 armed groups now occupy the east.
It was into this tinder-box that Ebola spilled over from an animal reservoir, most likely bats or apes, into humans. On 1 August 2018, a patient’s blood sample collected near Beni tested positive for Ebola. Oly Ilunga Kalenga, the DRC minister of health at the time, declared that the virus had arrived in northeastern DRC for the first time. “From day one,” says Ilunga, “I warned everyone that this would be a very bad outbreak because of conflict.”
Within a week, the Ministry of Health, the WHO and aid groups began establishing Ebola treatment centres. Health workers carted high-tech coolers filled with frozen Ebola vaccines into the rainforest, and epidemiologists from the WHO’s emergency-operations division arrived to investigate the spread of the disease. They were trying to learn how each individual got infected, and to search for anyone those individuals touched while sick. Health workers monitor these contacts for signs of Ebola, such as vomiting and fever, for 21 days — the incubation period of the virus. If they suspect an infection, they test and isolate people before it spreads. This cornerstone of the Ebola response, called contact tracing, is the key to stopping the virus’s transmission.
In a country with a strong, centralized network of doctors and public-health workers, contact tracing is manageable. But after decades of political instability, eastern DRC has no such system, and conflict makes it impossible to create one quickly. Between September and November last year, an armed group infamous for hacking civilians to death with machetes, the Allied Democratic Forces (ADF), slayed an estimated 55 civilians in and around Beni, and kidnapped dozens. Amid one attack, a rocket-propelled grenade hit the Okapi Hotel, where Ebola responders from the WHO were staying. It failed to explode, sparing their lives.
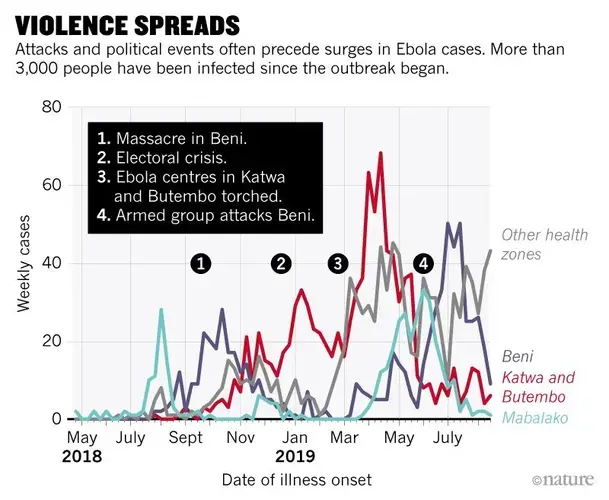
After each attack, front-line responders pulled back for their safety and the disease spread unfettered, with a surge of people dying from Ebola in the weeks following violence (see ‘Violence spreads’). Marta Lado, an infectious-disease physician at an Ebola centre in Beni, explains: “We start thinking we’ve got it under control, and then an attack happens and for three or four days, we can’t go into the community because it’s not safe, and the contacts disappear.”
By December, the outbreak had already become the world’s second-worst. Then things went from bad to worse. The president at the time, Joseph Kabila, barred more than one million people in Beni and Butembo — strongholds of opposition parties — from voting in the upcoming election. He blamed it on Ebola and the security situation, but many DRC citizens saw this as a thinly veiled attempt to retain power after an 18-year stranglehold on the presidency.
Volatile demonstrations erupted across the country. An Ebola centre was looted during one protest in Beni, but the real damage to the Ebola response was the politicization of the outbreak. The voting ban seemed to confirm rumours that this terrifying disease was a tool designed to disenfranchise the opposition and make money. After all, many Ebola responders came from the capital, Kinshasa, and from other countries. They stayed in comparatively upscale accommodations, and hadn’t cared about suffering in the region before. Some residents believed that these foreigners were importing Ebola to kill them, similar to the ADF, which arose seemingly out of nowhere and with international ties. As a doctor from Beni explained to me, “People think this is just another thing brought from outside to kill.”

Mistrust grew in January after the election, which was widely considered a sham. Kabila handed the presidency to a candidate who would later allow him to share power. On the night of 24 February, assailants burnt down parts of an Ebola treatment centre in Katwa. Three days later, they set another centre and its vehicles ablaze in Butembo. Immobile patients watched in fear from their hospital beds. Four people with Ebola fled into the forest. This attack coincided with the centre’s busiest hour, as daytime staff handed over to the evening shift. “They were such violent attacks. And they were planned,” says Trish Newport, an Ebola programme manager at the aid group Médecins Sans Frontières (MSF, also known as Doctors Without Borders). Fearing for their safety, MSF evacuated staff from Butembo and Katwa, and the WHO and the DRC Ministry of Health together filled the vacuum.
By early March, these groups had rebuilt facilities. But a week later, assailants ambushed one of the centres again, killing a police officer on duty. Tedros arrived at the bullet-pocked clinic later that afternoon to check on his staff. He announced that rather than running away, his legions would double down. Then, in April, Mouzoko was shot dead at another hospital in Butembo.
Tedros’s eyes well up with tears when he speaks of Mouzoko and his four children, now fatherless in Cameroon. Tedros flew from Geneva, Switzerland, to Butembo again just after the murder. “When I got there I couldn’t speak,” he recalls. “The staff were scared but at the same time, they told me they won’t be intimidated.” He made a decision: “We can show our respect to him by finishing Ebola.”
Tedros has put the WHO in the spotlight in the DRC. Throughout this year, the WHO has had around 700 of its staff in the cities and towns where Ebola is spreading. In contrast, the US Centers for Disease Control and Prevention (CDC) has had only about a dozen epidemiologists in the country, and they are not in the hot zone. Other aid groups that were at the forefront of the world’s largest Ebola crisis — in West Africa from 2014 to 2016 — such as MSF and the Red Cross, are helping, but in lesser numbers than the WHO.

Another difference in the current outbreak is that the WHO’s Ebola responders are almost all African — from the DRC, Guinea, Senegal and other French-speaking nations. Fall says it’s a sign of Africa’s growing ability to fight outbreaks on the continent. And he feels a personal sense of commitment: “I’m an African, and when I see my own people suffering, it is like my family is suffering and I have to do something.”
Yet by June, the WHO had conceded that it needed help from sister UN agencies that handle other aspects of humanitarian crises. The head of the UN peacekeeping mission in the DRC, David Gressly, stepped in as emergency Ebola coordinator. Some 3,000 UN troops had already been deployed to areas around Butembo and Beni, and Gressly tasked them with making the region secure for the Ebola response.
Tedros returned again that month to check on the transition with Gressly, and to depoliticize the outbreak by winning the support of key figures in the country. This included meeting the head of the DRC alliance of traditional authorities — a system of leadership that pre-dates colonization — and the head of the leading opposition party. “They all need to have the same position” on Ebola, he explained.
Although Tedros’s background is in science — he is an epidemiologist by training — it’s his years as a politician that surface as he navigates the complexities of DRC politics. He served his home country of Ethiopia as minister of health, and then as the minister of foreign affairs from 2012 to 2016. When the previous head of the WHO, Margaret Chan, announced she would be stepping down, Tedros campaigned for the position with support from former US president Jimmy Carter, among others. In July 2017, he became the first African to run the WHO. He pauses to think about what that means to Africans, then says, “When I visit, they understand that I understand their situation.”
A Delicate Operation
One hot June afternoon, a 52-year-old woman, Kyamwatsi Muswagha, returns from hours spent walking through the town of Aloya. She is one of hundreds of locals rapidly enlisted to do contact tracing, and she was searching for two dozen people who had been close to Ebola-infected individuals. That day in Aloya alone, these locals were supposed to monitor 1,500 people. Across North Kivu and Ituri, the daily number of contacts to trace was around 20,000.
Muswagha hands a stack of papers to a WHO epidemiologist who is already surrounded by piles of paper on a picnic table. Each sheet lists a contact’s name and checkboxes for fever, diarrhoea and other Ebola symptoms. When someone’s symptoms persist for a couple of days, Ebola responders investigate. But when I asked how the data in these stacks of paper are collated and analysed, I never got a clear answer. And Muswagha concedes that she misses some information. Some families hide; others say they’re fine, hoping she’ll go away. And the contacts on the list are only a fraction of those who might be infected. As of May, fewer than half of the individuals diagnosed with Ebola had been on a contact list. That meant that they weren’t offered Ebola vaccines and weren’t being monitored.
Across a clearing from the picnic table is a dusty, concrete building that is Aloya’s main health facility. In one of seven dank rooms, a woman draped in shadow holds her seven-year old daughter, who has hives and a high fever. A physician and epidemiologist, Dorine Ngono, explains that the woman refuses to let health workers take her child to the Ebola centre an hour away. On a mattress in another room lies a woman who delivered a stillborn baby a few days earlier. Stillbirths are a symptom of Ebola, so the responders want to test both her and the infant for the virus. The woman is distraught, however, and won’t reveal where she has buried her baby. Ngono has shed her WHO vest, and beads of sweat pool near her hairline. “People need to trust me, so I’m removing all things that could appear as a barrier,” she says.

When Ebola first hit a year ago, responders directed people who felt feverish to well-equipped Ebola centres. But they soon realized that many people weren’t going. As of May, roughly one-third of those with Ebola had died outside of the centres (O. Ilunga Kalenga et al. N. Engl. J. Med. 381, 373–383; 2019). And of those who did go, the WHO estimated that an average of around six days passed between the onset of symptoms and check-in. In the intervening time, the sick visited their pastors, healers, pharmacists and local health workers long before they travelled to specialized Ebola units. And responders found that these facilities were becoming sources of new infections.
So rather than ignore medicine shops and clinics like the one in Aloya, the WHO decided to prepare them for the deadly virus. So far, Ebola responders have identified more than 1,000 such facilities in North Kivu, and they say they’re offering Ebola vaccines to the people working there. But 156 health workers have been infected in this outbreak, suggesting that something has gone awry. Bringing the clinics up to speed is labour-intensive, says Marie-Roseline Darnycka Bélizaire, a WHO field coordinator in Butembo. “You should see some of these places,” she says. “The floor is earth; the walls are old, decayed wood; some have no running water and the ceiling is so low you can’t stand up. And the main room with patients is about the size of one of our bathrooms.”
Ngono says that she and other outside specialists cannot just take the reins from local health workers, either. “We have to train them and let them do the work,” she says, “and give them a bonus in their salaries to do it.”
Criticism Amid Chaos
Ngono eventually convinces the woman who had given birth to have her blood tested. She is negative. That’s a good sign, as is the rising rate of people getting vaccinated in Beni. But good news always seems to be followed by bad. In July, two local Ebola responders were killed by their neighbours, who allegedly envied them for finding employment in the response. The following week, a woman with Ebola travelled to Uganda to sell fish, vomiting along the way. And an evangelical pastor with Ebola took a two-day bus ride from Beni to Goma, a city of two million with an international airport. From there, the virus could feasibly hitch a ride to Dubai, Belgium or Beijing.
The risk of the epidemic spreading internationally was growing larger every day, along with a chorus of analysts and researchers who criticized Tedros for not declaring the outbreak a ‘public-health emergency of international concern’, or PHEIC. Some observers worried that the WHO was repeating mistakes from the West African outbreak. Back then, critics had accused the organization of ignoring signs of an escalating crisis, and initially shirking its responsibility to assist Sierra Leone, Liberia and Guinea — countries where the infrastructures are too weak to handle the outbreak without help. An independent audit of the WHO’s actions in 2015 concluded that without significant change, the agency would no longer be considered the pre-eminent guardian of global public health.

Such opinions matter because the WHO is kept afloat by donations from governments and philanthropists, who must be convinced of the value of their investments. In response to the charges, in 2016, the WHO created an emergency operations programme that included a contingency fund of a proposed US$100 million to be tapped quickly in a crisis. When Tedros took office, he promised to strengthen the operation’s capacity. The number of WHO emergency responders in Africa has more than doubled from 100 in 2016 to more than 250 in 2019.
Money from the contingency fund allowed the WHO to deploy epidemiologists and supplies to eastern DRC as soon as the Ebola outbreak started. And Tedros has consistently called the situation an emergency — even though he and his advisers delayed calling it a PHEIC, worrying that this could backfire if countries responded by closing borders. “Whether or not you label it a PHEIC does not matter for us,” says Newport at MSF. “What matters is that the WHO has been present and is working hard in one of the most complex emergencies we’ve seen in a long time.”
But by July, the WHO had burnt through its contingency fund, forcing it to scale back support in other disasters around the world, such as a surge of childhood HIV in Pakistan. Come August, only $8.7 million was left in the pot, and donors weren’t giving enough additional money. For the first half of 2019, they had given the WHO less than half of the $98 million it requested for the Ebola response. And the agency estimates that the response for the second half of the year will cost nearly $300 million. On 17 July, Tedros sounded the alarm, declaring the outbreak a PHEIC.
Suddenly, the media was all over the epidemic. But with renewed attention comes added scrutiny. Some officials and researchers bemoan a lack of epidemiological information — the type of data collected in piles of paper on the picnic table in Aloya. Either they don’t exist or the WHO isn’t sharing them, suggests Jennifer Nuzzo, an epidemiologist at Johns Hopkins University in Baltimore, Maryland. Intelligence on how many contacts aren’t being monitored daily, or on how many health workers refuse vaccines, could help scientists to pinpoint gaps in the response. Nuzzo says she understands the WHO needs the money, “but we need to make sure we’re not trying to fill a bucket with a hole in it”.
In May, an independent committee published a different set of concerns about the WHO’s emergency response. The group called the operation impressive, but expressed concern over public-health messaging. The committee had spoken with community leaders in Butembo, for example, who said that Ebola is spread by dirty hands when, in fact, it passes through the bodily fluids of infected people. The report also said the WHO was overstretched, and suggested that armed guards around Ebola centres and vaccine stations could intimidate communities.
Tedros acknowledges gaps in his agency’s response, but notes that the WHO and the DRC government had rapidly contained an Ebola outbreak just before this one in western DRC, a more stable region of the country. “We’re trying to do better,” he says, “but we also need to protect our responders from ambushes — we’ve already lost seven.” Another 60 have been injured in targeted attacks just this year.
And Tedros is trying to respond to complaints from people in the DRC, too. Chief among their issues is what they see as neglect for other pressing health problems, such as measles, malaria and malnutrition. So now, the WHO, the DRC Ministry of Health and aid groups are providing more general health care, to show that they want to help. “When I visit, people ask me why I care about Ebola alone when they have other killers,” says Tedros, “and I am embarrassed that the answer to that question is that the international community is only concerned if something can cross the border.”
Fragile States
Back in June, on a warm evening filled with birdsong in Beni, medical anthropologist Julienne Anoko sits by a pool at the Okapi Hotel. A silhouette of a sniper’s nest on the roof is the only reminder that the city is under siege. Anoko was staying here last November, when bullets blasted through the plaster of her room. She will sleep in the same room tonight, but she seems relaxed, having just returned from several days spent deep in the forest.
Anoko is renowned for such missions. In 2014, she calmed tensions in Guinea by introducing a ceremony for burying Ebola-infected corpses that appeased mourners and infectious-disease specialists alike. As soon as the DRC outbreak began, the WHO flew her to North Kivu, asking her to lead a team of 40 other social scientists. Their goal is to change the behaviour of communities so that people will permit invasive measures, such as Ebola responders dressed in white space suits dousing belongings with chlorine solution.
On Anoko’s most recent trip, she had ridden motorcycles through the jungle with a handful of other Ebola responders. At one town known to have housed several people with Ebola, a community refused to allow the group to enter. “I tried to talk with the mothers, but they just stared at me,” Anoko says. As people gathered to watch, she asked a boy for his name. He sassily said he was Lionel Messi, the Argentinian football star. So she told him to call her Cristiano Ronaldo, and then challenged him to arm-wrestle her for the World Cup. “So we wrestled,” she says, “and everyone was watching and laughing.” Anoko returned the next day with a football as a gift. And then the community agreed to let in health workers with vaccines.

“People are so afraid. They don’t know if we might be terrorists who want to kill them,” she says. “So we just show them that we are human — mothers, fathers, sisters, brothers — we explain why we want to help.” These conversations work, she says; they only take time. And when armed groups ambush, people run for their lives. “It’s like Sisyphus,” says Anoko, lifting her arms. “You are pushing this boulder and when you think you’re at the top, there’s an attack and the rock rolls down again.”
In July and August, armed groups killed and abducted more DRC civilians. In response, residents of Beni held a protest directed at UN troops and the authorities who had failed to protect them. The responders stayed indoors that day. As of 7 September, Ebola had infected roughly 3,080 people, killed 2,060 and spread 700 kilometres to the war-weary province of South Kivu, bordering Burundi and Rwanda.
A prospect that terrifies specialists on pandemics is that the outbreak in eastern DRC represents a type of complex emergency that no health agency will ever be able to extinguish rapidly. Ebola and other deadly pathogens will keep spilling over from animals into humans, and the ever-increasing mobility of people will help infections spread. It’s no coincidence that the world’s two largest Ebola outbreaks have exploded in densely populated regions of countries with ineffective health systems, extreme poverty and a history of exploitative colonization and conflict.
Chikwe Ihekweazu, the director of Nigeria’s Centre for Disease Control, reflects on Ebola responders who have been stationed at the epicentre of the outbreak for months. “I know how hard my colleagues in the field are working — 18-hour days, losing track of the weekend,” he says. “In some ways, they are paying for all of us ignoring the situation in this part of the continent for many years.”
This outbreak will eventually end, but it could cost tens of thousands of lives and billions of dollars. When Tedros took the helm at the WHO, the top of his agenda was not emergency response, but universal health care — delivering basics such as antibiotics, vaccines and a network of labs to identify infections. Curbing Ebola should be straightforward with political stability and a robust health system, Tedros says. But in their absence, a cycle of tragic, multimillion-dollar health disasters will continue to flourish in the DRC, Yemen and other fractured regions of the globe. “As long as places are this vulnerable, this will keep happening,” he says. “We will fix Ebola — and it will come back tomorrow.”
 in Katwa. Image by John Wessels. Democratic Republic of Congo, 2019.")
Education Resource
Meet the Journalist: Amy Maxmen
The Democratic Republic of the Congo experienced the second largest Ebola outbreak in history. But...


