She leads the fight against cholera, a deadly infection that has surged globally.

Bangladesh is leading the fight against this ancient scourge, and vaccine researcher Firdausi Qadri is on the front lines.
A version of this story appeared in Science, Vol 387, Issue 6734.
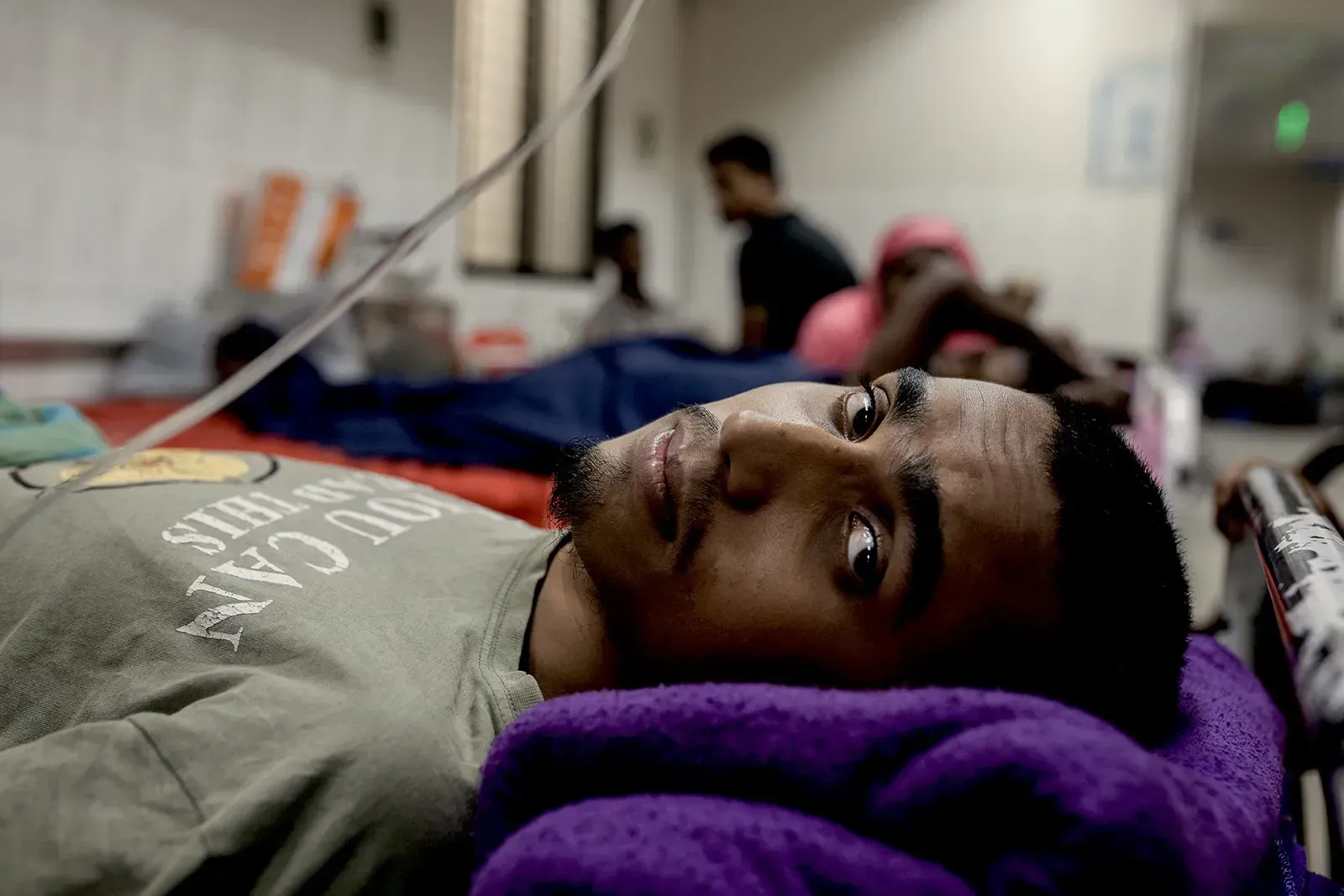
Dhaka, Bangladesh—Mohammad Abu Raihan Shanto had suffered from uncontrollable diarrhea for 3 days, until he became so weak he couldn’t walk and relatives took him to a hospital. Now, the 19-year-old madrassa student was hooked up to an intravenous drip to rehydrate his body, and he felt slightly better, although he was still weak and his eyes looked hollow. “I thought I was going to die,” Shanto said through an interpreter as his mother and a younger brother looked on.
Shanto’s hospital bed, like those of scores of other patients in the large hospital hall, had no sheets but a plastic cover, and a hole in the middle with a blue bucket underneath. That allowed patients to empty their bowels without getting up. (“He is having a discharge right now as we talk,” the interpreter helpfully said as Shanto briefly closed his eyes.) About 10 meters away, a man sitting on his bed vomited loudly.
They had come to the right place: a hospital in central Dhaka operated by the International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B). It is known internationally as a crown jewel of South Asian science and locally as the best place to go if you have severe diarrhea caused by cholera or one of the many other intestinal bacteria flourishing in Bangladesh. (Rather than use the tortuous acronym, ICDDR,B’s website suggests to visitors: “Just ask your driver for the cholera hospital.”) Untreated cholera can kill within hours through catastrophic dehydration, but here treatment—primarily rehydration—is free, and most patients are discharged within 24 hours.

As a nonprofit journalism organization, we depend on your support to fund more than 170 reporting projects every year on critical global and local issues. Donate any amount today to become a Pulitzer Center Champion and receive exclusive benefits!
The center is also the domain of Firdausi Qadri, “the queen of cholera,” as Philippe Barboza, of the World Health Organization (WHO), calls her. Qadri, who heads ICDDR,B’s Mucosal Immunology and Vaccinology Unit, housed five stories above the hospital, has spent her career studying a range of enteric diseases, but most of her work has been on cholera, and it has given her near-legendary status. Qadri is “a scientific giant,” Swedish vaccine researcher Jan Holmgren wrote in 2021. A “godmother” to the field, says Julia Lynch, who heads the cholera program at the International Vaccine Institute (IVI) in Seoul, South Korea, which has close ties with ICDDR,B. “She’s phenomenal,” Lynch says. “An amazing, compassionate, hardworking person who’s also a terrific scientist.”
Much of Qadri’s work has focused on demonstrating the benefits of a generation of simple, cheap oral cholera vaccines and advocating for their use. The rollout of these vaccines, first developed by Holmgren at the University of Gothenburg more than 4 decades ago, has been agonizingly slow, in part because there’s no money in making vaccines for diseases of the poor, but also because many in the public health community were skeptical. After all, vaccines do little to address cholera’s root cause: the lack of clean water and sanitation that help Vibrio cholerae (V. cholerae) thrive.
It wasn’t until about a decade ago that countries began to use vaccination more widely, in part thanks to Qadri’s advocacy. “She has been a leader on oral cholera vaccines for a very long time, and has just carried out a whole series of studies that demonstrate how you can do it,” says David Sack, a veteran cholera scientist at the Johns Hopkins Bloomberg School of Public Health.
But as the teeming hospital ward at ICDDR,B showed, oral vaccines have not eliminated cholera—not by a long shot. An international stockpile that distributes the vaccines to poor countries with support from Gavi, the Vaccine Alliance has too few doses to meet the global demand. The Bangladeshi government, struggling with many other urgent health problems, is not investing in vaccination. Complicating matters, the vaccine offers protection for just a couple of years. Progress in providing clean drinking water and sanitation has been slow as well, both in Bangladesh and other cholera-prone countries.
As a result, several plans to dramatically curtail cholera, both globally and in Bangladesh, are off track. In 2022, Dhaka saw its worst outbreak in more than 25 years; the ICDDR,B hospital treated more than 42,000 patients in a 41-day period. Outbreaks have surged globally in the past 2.5 years as well, driven in part by conflict and climate change. “It’s frustrating,” Qadri says.
When Science visited in June 2024, the hospital had just dealt with another big influx of patients, peaking at more than 1,300 a day. Many had cholera, although few were actually tested, as the treatment for severe diarrhea is similar regardless of the cause. Staff had erected two air-conditioned tents in a parking lot to receive patients. More patients were parked in hallways and corridors. (You’d expect the place to smell horrible, but it didn’t: Cleaning crews frequently replaced the buckets and mopped the tiled floors.)
The institute now faces another, urgent problem: Last week, it said it had laid off more than 1,000 employees across 10 projects and studies in response to a 3-month “freeze” in U.S. foreign assistance, which helps support it. Qadri declined to comment on the move, and an ICDDR,B spokesperson would not say whether her research would be affected. He said, “We hope to resume our activities soon.”
Over lunch last summer, Qadri said she remained an optimist, confident cholera can be vanquished—and that science can help solve other public health problems in her tumultuous country, which saw its authoritarian government overthrown in a surprise revolution last year. At age 73, Qadri works 6 long days a week at ICDDR,B and at a private institute she co-founded a decade ago to address neglected health needs and train young scientists. “I want to do so much,” Qadri said before she got up for her next meeting. “Do you think I’m a madwoman?”
It's no coincidence that “the mecca of cholera research,” as Holmgren calls it, is in Bangladesh. Bacteria emerging from the brackish water of the Ganges River delta are believed to be the origin of six of the seven cholera pandemics that have washed over the globe the past 200 years, killing tens of millions of people, stoking fear and panic, and inspiring novels and movies. (The third pandemic, from 1846 to 1860, struck London, where physician John Snow famously showed cholera was carried not by bad air, but by contaminated water. The seventh began in 1961 and is ongoing.)
ICDDR,B was established as the Cholera Research Laboratory in 1960 by the Southeast Asia Treaty Organization, a U.S.-backed group aimed at stopping the rise of communism. During its first 60 years, the lab was led by foreign scientists, who helped bring in collaborations, expertise, and funding. (The center’s hallways are lined with photos of famous visitors, including Hillary Clinton and Melinda French Gates.) In 2021, nutrition scientist Tahmeed Ahmed became the first Bangladeshi to head the center.
In the 1960s, ICDDR,B played a pivotal role in the development and testing of oral rehydration solution, a cheap, simple mix of glucose and salts that can be dissolved in water and given to diarrhea patients to replace lost fluids and prevent dehydration. “Bangladesh’s gift to the world,” as Ahmed called it, became a first-line treatment globally, saving millions of lives. The institute has since expanded into malaria and other mosquito-borne diseases, HIV/AIDS, malnutrition, child and maternal health, and other medical challenges facing Bangladesh. But it also helps prevent diseases that cross borders, says U.S. cholera scientist John Clemens, who headed ICDDR,B from 2013 to 2021. He predicts halting financial support “will be very expensive for the U.S. in the long run.”

Qadri was born in Dhaka when Bangladesh was still a province of Pakistan. Her parents divorced when she was young, and she was mostly raised by her grandparents. Her grandmother insisted she pursue a good education, which was unusual at the time in Bangladesh’s Muslim-majority society. “Girls have to have their own profession, their own education, and their own earning power,” Qadri says her grandmother told her. Qadri’s older sister, who became a physician, urged her to study “something more modern, more trendy, like molecular biology, microbiology, or biochemistry,” Qadri says. “No need for another doctor in the family.”
Her studies at Dhaka University, where she got a master’s degree in molecular biology, were interrupted for 9 months by the brutal war that led to Bangladesh’s independence in 1971. Hundreds of thousands, perhaps millions, were killed by the Pakistani military and affiliated militias, including many students and academics. Qadri’s family came out unscathed, but “when it was over we didn’t know whether to smile or cry because so many people we knew were dead.” She says the episode strengthened her love of country.
In 1977, Qadri moved to the United Kingdom with her husband, also a scientist, to do a Ph.D. in biochemistry and immunology at the University of Liverpool. She loved life there—the colonial era had instilled a deep appreciation of England in her family, she says—but the couple returned to Bangladesh in 1980 to help rebuild the destitute country. In 1986, she joined ICDDR,B as a postdoc. Since then, she’s worked on many intestinal pathogens common in Bangladesh, including Shigella, Escherichia coli (E. coli), and rotavirus, but her main focus has been cholera.
On a warm Tuesday morning, Qadri showed Science around a slum in Mirpur, a neighborhood in northern Dhaka, with a few younger scientists and assistants in tow.
The streets were lined with gray concrete apartment blocks. Inside, families of five or more lived in a single room, their possessions stacked against the walls, a big TV screen hanging over the bed. Qadri stopped occasionally to make small talk with residents, inquire about their children’s health, or ask to see their vaccination cards.


The neighborhood is one of ICDDR,B’s main research sites. Qadri led a study here in more than a quarter-million people, published in 2015, to show that mass cholera vaccination among the urban poor is feasible. Today, one study is testing the duration of the vaccine’s protection in children. There are also trials of new vaccines against typhoid and Shigella, and one to explore whether vaccinations against cholera, typhoid, measles, and rubella can be combined.
It’s not hard to see why pathogens that travel the fecal-oral route could thrive in the neighborhood. Most households have running water, disinfected at the source with chlorine, but the supply is uneven. Occasionally, water pressure drops, allowing dirty water to leak into the neighborhood’s pipes and tubes. Multiple households can share a single kitchen and a single foul-smelling toilet, meaning anybody infected with cholera can easily expose many others.
Providing clean drinking water, sanitation, and hygiene—WASH in cholera jargon—is the best way to prevent the disease. “It’s why you don’t have cholera in London and New York anymore,” Qadri says. It’s also a very tall order for a poor, extremely densely populated country. Bangladesh, less than one-third the size of Spain, has more than 170 million inhabitants, more than 20 million of them in greater Dhaka.
Scientists have long tried to tame cholera with vaccines instead. The 20th century brought injected vaccines made of whole, killed V. cholerae cells. But they sometimes had severe side effects, and the injections could hurt, recalls Qadri, who got them as a child: “It was so painful that we would hide under the bed.” Worse, large-scale trials in the 1960s showed these vaccines provided poor protection: 50% at most, for just a few months, and only in adults. WHO stopped recommending them in the 1970s.
At his lab in Sweden, Holmgren pioneered a new strategy: an oral vaccine that would elicit so-called mucosal immunity in the lining of the gut, blocking the bacterium where it attacks. His vaccine also contained whole killed V. cholerae cells, but they were combined with the so-called B-subunit, a part of the microbe’s toxin protein, and given orally rather than injected. A 1985 study in Bangladesh led by Clemens showed two doses offered about 85% protection during the first 2 years.
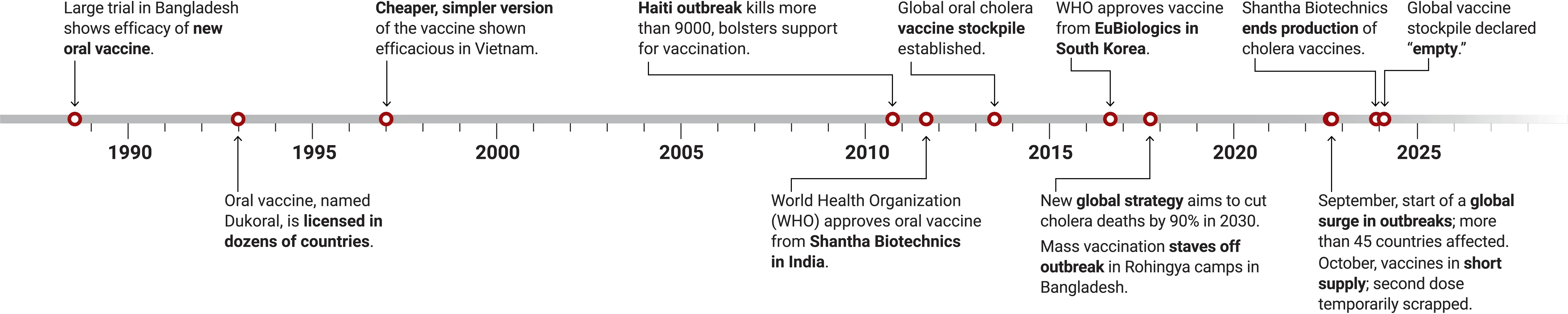
The vaccine, named Dukoral, was licensed in many countries in the early 1990s and is produced today by Valneva, a France-based company. But it has always remained a “traveler’s vaccine” used by people from developed countries. “It was just too complex and too expensive to work in mass vaccination campaigns,” Lynch says. The stomach’s acids break down the B-subunit, so recipients need to take the vaccine with 150 milliliters of a fizzy buffer solution, which makes shipping and distributing it pricey and cumbersome.
But the toxin subunit was not essential. Holmgren helped transfer the technology to Vietnamese researchers, who dropped the subunit and tested a vaccine made of only killed cells—but still taken orally. Trials published in 1997 showed two doses provided about 66% protection. A team led by Clemens, who led IVI between 1999 and 2011, further refined the vaccine and then transferred the technology to Shantha Biotechnics in India, which agreed to produce it cheaply for use in developing countries. For their work on the vaccine, Holmgren and Clemens won several prestigious awards, including the Albert B. Sabin Gold Medal.
Within WHO and elsewhere in the global health community, however, some saw oral vaccines as a technological fix and a distraction from WASH measures—which prevent many other waterborne diseases—and from early detection and proper treatment. “There were always discussions between the WASH people and the vaccine people,” Qadri says.
A long, winding journey
Oral cholera vaccines first proved their mettle almost 4 decades ago, but their development and introduction has been a long, slow process. Today, as outbreaks are raging in dozens of countries, there is a huge shortage of doses.
Vaccination remained rare, and Qadri’s frustration grew. Sometimes she could hear patients retching and vomiting in the hospital from her office, she says, “and I was very disappointed. I felt my work didn’t have any meaning.” To expand vaccine use, she helped organize a 2007 meeting in Dhaka that brought together governments, global health agencies, and vaccinemakers. She also won support from the Bill & Melinda Gates Foundation for the feasibility study in Mirpur.
A turning point came in October 2010, when cholera broke out in Haiti, 10 months after an earthquake that killed 200,000 people. Hundreds of thousands got sick and more than 8,000 died in the first year. The tragedy drove home that working on WASH was all well and good, Holmgren says, but vaccines could save lives in the meantime. “It was absolutely decisive,” he says. (That the outbreak originated in a camp for U.N. peacekeepers may have helped sway opinions within WHO, itself a U.N. organization.)
In 2013, a consortium of global health organizations set up an oral cholera vaccine stockpile that allowed countries suffering from a cholera outbreak to apply for an emergency shipment. Initially, the stockpile contained only Shantha’s vaccine, but in 2016 it added a second, very similar vaccine produced by South Korea-based EuBiologics with help from IVI.
In 2017, a humanitarian crisis in Bangladesh showed just how powerful the vaccine stash could be. Genocidal violence against the Rohingya, a Muslim minority in Myanmar, led an estimated 700,000 people to flee across the border, into the southern tip of Bangladesh. The Bangladeshi government and international organizations scrambled to provide safety and shelter in massive camps near the city of Cox’s Bazar. “It was such a sad sight,” says Qadri, who flew to the area within weeks after the influx and has since visited dozens of times. “There were people sitting everywhere, in the rain and mud, with such a vacant look on their face.”
It was also a cholera epidemic waiting to happen. “My heart told me we had to do something quickly,” Qadri says. With help from ICDDR,B, the Bangladeshi government submitted a request for 900,000 doses to the stockpile in late September 2017. It was approved within 24 hours, and in November more than 200 vaccination teams swarmed out across the camps. The outbreak didn’t happen. Since then, there have been eight additional vaccination rounds in the camps, whose population has swollen to well over 1 million.
Optimism rose about the potential of the oral vaccines. In 2017, a broad coalition of agencies and groups called the Global Task Force on Cholera Control published a plan for a 90% reduction in cholera deaths by 2030 that relied on improving WASH and early outbreak detection but also called for “large-scale” use of vaccines. “As many as 20 countries could eliminate the disease as a threat to public health by 2030,” the plan said. Hot spots such as Bangladesh, which occasionally seed outbreaks elsewhere, would get special attention. (“There is no controlling cholera without controlling cholera in Bangladesh,” Clemens says.) The country’s own National Cholera Control Plan for 2019-2030, which Qadri helped write, set a similar 90% reduction target for the country, by 2030.
In 2018, Gavi’s Board approved a proposal to make vaccines from the stockpile available not just for “reactive” campaigns—in response to outbreaks or humanitarian crises—but also for “preventive” campaigns in places like Bangladesh where the disease strikes every year. To be eligible for support, countries would have to strengthen surveillance, identify areas of intense transmission, and submit a detailed multiyear plan.
Bangladesh—and Qadri—embraced the idea. The country wrote an application for 100 million doses of vaccine, which a Gavi review panel approved in November 2023 and is currently being finalized.
But things haven't gone according to plan. Cholera cases did decline globally for a few years after the 2017 road map, but the COVID-19 pandemic wiped out part of those gains. Then came the massive outbreak in Bangladesh in 2022, and others in war-torn countries such as Sudan, Syria, and the Democratic Republic of the Congo. Climate change, and the extreme weather it favors, made things worse. Droughts, which can lead people to resort to unclean water, triggered outbreaks in Zambia and Zimbabwe; floods, which can destroy infrastructure and contaminate drinking water, did so in Kenya.
The stockpile hasn’t kept up. In 2022, French pharma giant Sanofi, the parent company of Shantha, ended the production of cholera vaccines, despite protests from WHO. (Critics suspect Sanofi didn’t deem the vaccines profitable enough; a company spokesperson says Sanofi only produced 10% of doses globally anyway and supply from other producers was set to grow.)

That has left EuBiologics as the only supplier, and it only produced about 50 million doses last year, far short of the demand. Allocating doses has become “like Sophie’s choice,” says Barboza, WHO’s representative on the international group managing the stockpile. In late 2022, the panel decided to temporarily switch to a one-dose regimen, which a 2016 study by Qadri in Bangladesh had suggested offered reasonable protection, although not in children under age 5.
Bangladesh has an alternative source of vaccine, at least on paper: IVI has also transferred its vaccine technology to Incepta Pharmaceuticals, which has a big, state-of-the-art production facility in Dhaka’s outskirts. But the government, which is facing many other health challenges, hasn’t deemed cholera urgent enough to buy from Incepta. The company can’t supply the global stockpile either, because WHO has not yet approved its version of the vaccine. “We are completely locked,” says Abdul Muktadir, Incepta’s frustrated CEO. “We can’t sell anything.”
Things are now beginning to look up. EuBiologics recently increased its production capacity and may produce more than 70 million doses this year, and the stockpile is back up to 5 million doses, seen as the minimum needed to address emergencies. “We’re in a much better place than we were a year ago,” says Gavi cholera expert Allyson Russell. Two other companies, in SouthAfrica and India, are expected to bring similar vaccines to the market in 2026, which should further ease shortages. Still, when Bangladesh might get its 100 million doses is unclear. “It’s sad when you have a way to prevent disease and you can’t use it,” Qadri says.
Bangladesh is at a major crossroads. In August 2024, student protests toppled the country’s autocratic government, which had tried to suppress them with deadly violence. Now, 84-year-old Muhammad Yunus, a microfinance pioneer and Nobel Peace Prize winner, is leading an interim government and heading the effort, along with students, to write a new constitution. Recent reports have documented the disappearance of thousands of political opponents and widespread corruption under Sheikh Hasina, the ousted prime minister.
Qadri says Hasina had supported her work, and the former prime minister gave her the Independence Award, the nation's highest honor, in 2023. But, “I’m not a political person,” Qadri said. “There are young people now taking over. I’m waiting to see what will happen.”
She did take heart from the progress Bangladesh has made. Its economy has grown at more than 6% annually for many years, in part thanks to a burgeoning garment industry that has provided millions with a living wage and made women more independent. In other positive signs, the birth rate has plummeted, from 3.6 children per woman in 1995 to below two, and the share of people living below the national poverty line has dropped steeply.
Qadri hopes the new government will devote more resources to science. ICDDR,B enjoys support from many foreign sources—“Without the Gates foundation, I would be nothing,” Qadri says—but the country’s own expenditure on R&D is just above 0.3% of gross domestic product, among the lowest in the world. In the meantime, Qadri has set up her own initiative—“my gift to the country,” as she calls it. Using money from her awards, including €500,000 from a prestigious French prize in 2012, she and her husband in 2014 launched the Institute for Developing Science and Health initiatives (IDESHI). “I wanted to create something different, something new,” she says—a place for training young scientists whose culture she could shape herself. Today IDESHI employs more than 60 people working on a broad range of neglected health issues in Bangladesh. For example, a Gates-supported project aims to increase awareness of cervical cancer and encourage vaccination against the human papillomavirus (HPV), which causes it. It’s a delicate task, because HPV is transmitted sexually. “In our culture we do not talk about sex,” Qadri says.

Another project aims to prevent thalassemia, a blood disorder caused by a recessive gene that many people unknowingly carry. Marriages between cousins, common in Bangladesh, increase the risk. The project is encouraging people to get tested and, if they have the gene, avoid marrying another carrier. “A woman often hesitates to express that she is a carrier,” says Kasrina Azad, the medical officer leading the project. “In our culture, it’s like she has bad blood or something. So she faces a lot of stigma.”
Forty percent of the staff at IDESHI are women, an unusually high number in Bangladesh. Qadri herself has undoubtedly “blazed a trail,” Lynch says. “I’ve seen her interact with government officials, and everyone is just like, ‘Oh, you don’t mess with her,’” she says. “She’s so respected, they listen to what she has to say.”
On 11 January, Qadri headed back to the Rohingya camps, where workers were about to launch another round of cholera vaccinations, in response to a worrisome rise in cases. The battle against Bangladesh’s ancient scourge was continuing—and Qadri would never give up her role in it, she said: “Do I look like I can retire?”