Story
![]() March 1, 2019
March 1, 2019
A Prescription for Madagascar’s Broken Health System: Data and a Focus on Details
Country:



IFANADIANA IN MADAGASCAR—Matt Bonds was young and idealistic when, as a postdoc, he set out with economist Jeffrey Sachs, a rock star in the development world, in his quest to end poverty. But the Millennium Villages Project on which they worked—a package of interventions from seeds to schools to clinics designed to improve livelihoods and health in impoverished African villages—came under withering criticism, including for a research design that made it impossible to gauge the project's impact. Sachs, of Columbia University, was excoriated and Bonds, who was skeptical of the methodology from the start, was deeply frustrated.
He was still young and idealistic when, at age 32, he went to Rwanda to join Harvard University's Paul Farmer, whose work with Partners In Health (PIH) was immortalized in Tracy Kidder's book, Mountains Beyond Mountains. In Haiti, Farmer and PIH co-founder Jim Yong Kim pioneered an innovative approach to bring health care to people who had nothing. Now, PIH was helping the Rwandan government rebuild its health system, which had been shattered by the 1994 genocide.
Bonds says that work, in three hard-hit rural districts, was "off the charts successful," noting that under-5 mortality—a key indicator of population health—dropped 64% in 5 years. But so much was changing in Rwanda at the time—international aid was pouring in, the economy was booming, and strongman President Paul Kagame had restored a tough order—that some questioned how big a role PIH played. "We didn't have the data" that could document our impact, Bonds laments. "We didn't have a true baseline. The data system was not in place until 6 years after the project started."
This time, Bonds, a polymath with Ph.D.s in economics and ecology who is now at Harvard Medical School in Boston, is determined to get it right, with meticulous data gathering and rigorous analysis. He is working in a remote district in Madagascar, one of the poorest countries in the world, where maternal and childhood mortality rates are shockingly high and half the children are stunted from chronic malnutrition.
With an eclectic group of partners and donors, including two Harvard-trained astrophysicists and a global tuberculosis expert, Bonds co-founded a nongovernmental organization (NGO), PIVOT. Its goal is to devise and test an affordable and effective health care system that could ultimately be scaled up to cover all of Madagascar and, perhaps, be adapted for other countries.
Like Sachs and Farmer, Bonds and his colleagues at Boston-based PIVOT are convinced that the single interventions that capture most international dollars, such as bed nets for malaria or targeted HIV/AIDS programs, although essential, are simply not enough. In a place as broken as Madagascar, you must tackle the whole messy health system with all its moving parts. And that means sweating the small stuff along with the big—ensuring there are trained surgeons and essential medicines, but also such quotidian things as gas for the ambulances and a paycheck for the pharmacist.

Other health system efforts are also underway. But PIVOT's almost obsessive focus on data sets it apart. PIVOT has been collecting mounds of it from day one, starting with a baseline study of 8000 people, with follow-ups every 2 years, and a monitoring and evaluation program that tracks more than 860 indicators so the team can document what works, fix what doesn't, and create a model health system that others can replicate.
"We wanted it to be done in a scientifically rigorous way," says Jim Herrnstein, the astrophysicist who, with his astrophysicist wife Robin, are two of the four co-founders of PIVOT and the group's biggest donors. "This is not a vision of rainbows and ponies."
"The degree to which PIVOT measures and holds themselves accountable for impact is remarkable and unusual," says Peter Small, head of the Global Health Institute at the State University of New York (SUNY) in Stony Brook. And so far, it seems to be paying off. In a paper last spring, PIVOT researchers reported that in just 2 years, under-5 mortality in their pilot area dropped nearly 20% and neonatal mortality fell 36%—results Small calls "impressive." The analysis has also revealed where improvements have been less dramatic, which has prompted PIVOT to rethink some strategies.
With its focus on data and evaluation, "PIVOT is really doing this right," says Katherine Burke, deputy director of Stanford University's Center for Innovation in Global Health in Palo Alto, California. "It is addressing all the failures in global health pilot projects."
Stunning beauty, abject poverty
The name Madagascar conjures up images of lush rainforests, ring-tailed lemurs with their impossibly shiny eyes, and chameleons of ever-changing hues. The island is indeed magical, among the hottest of all biodiversity hot spots with as much as 90% of its species found nowhere else on Earth.
Yet this biological richness obscures the desperate conditions in this country of 24 million. At least 90% of the original forest is gone, and 90% of Malagasy people live on less than $2 a day. Just 11% of the rural population has access to an improved latrine; 34% to clean water, according to UNICEF. No wonder diarrhea is one of the top killers of children, along with pneumonia and malaria. Malnutrition rates are the fourth highest in the world.
Forgotten diseases take a heavy toll: schistosomiasis, filariasis, leprosy, even plague, the Black Death of the Middle Ages, which returns like clockwork every fall—last year in the most fearsome outbreak ever.

One of the biggest barriers to health in Madagascar is simply the terrain. The same stunning geography that gave rise to such unparalleled speciation has left people isolated in remote villages, far from any clinic. Here in Ifanadiana district where PIVOT works, half the population lives in communities that can be reached only by foot or motorbike, hours or days off the main road.
And there are few outside dollars to help. Donors have long been reluctant to invest because of the country's history of political turmoil and corruption, and a 2009 coup cemented those fears. Madagascar became an international pariah, ineligible for foreign aid, and annual per capita spending on health plummeted to $14, the lowest in the world. After democratic elections in 2013, foreign aid began to trickle in again, and humanitarian groups have returned to parts of the country.
Crazy connections
PIVOT came about through a web of "crazy connections," as Robin Herrnstein describes it, at the center of which is primatologist Patricia Wright. Thirty years ago, in a remote montane rainforest in southeastern Madagascar, Wright discovered one lemur species and rediscovered another thought to be extinct. She persuaded the government to create Ranomafana National Park to preserve the rainforest and her beloved lemurs, and now splits her time between the research station she runs there, Centre ValBio, and SUNY Stony Brook. In 2009, Wright was looking for money for a new building at the research station when she was introduced to the Herrnsteins.
Robin and Jim Herrnstein met at Harvard as graduate students, both studying massive black holes. She went on to Columbia, and he had lined up a job at the University of California, Berkeley. But he changed course when he gave a talk at the secretive and hugely successful quantitative hedge fund Renaissance Technologies on Long Island in New York, where almost all the analysts are physicists, mathematicians, and statisticians. The fast pace and freewheeling intellectual culture drew him in, and he joined the firm. "We had been starving graduate students. Suddenly, we found ourselves in a position to help," says Robin Herrnstein, who left academia to start a family—one that rapidly expanded when the third child they were expecting turned out to be identical triplets.
Wright invited the Herrnsteins to Ranomafana. They were wowed by the rainforest, now a UNESCO World Heritage Site, with its rich and endangered biodiversity, and the science underway at Centre ValBio. And they were struck by the extreme poverty right next door. "You can't describe the beauty and the suffering in words," Robin Herrnstein says.
The couple agreed to fund the new building—but only if it included a biosafety level 2 infectious disease lab, "so researchers could study not only lemurs and frogs, but what is affecting the people," Robin Herrnstein explains. And they began to look for ways to do more.

At a gala event for SUNY Stony Brook donors, the couple was seated next to the guest of honor, actor Edward Norton, who helps run a conservation project with the Maasai in Kenya. They told him about their still-nascent idea of bringing health care to an isolated corner of Madagascar. "You've got to meet my brother-in-law," responded Norton, who then introduced them by email to Bonds, who is married to Norton's sister, Molly.
Bonds, now 42 and still idealistic, inhabits two worlds, the cerebral and the practical. A theoretical modeler, he made a name for himself with Sachs for his work on how cycles of infectious disease keep people trapped in poverty, and he has spent much of his career since then parsing which of the two comes first. Farmer and PIH helped bring him down to Earth. "It was like jumping off a cliff. … There was nothing I had learned as an economist that shed light on what it actually takes to do stuff," he recalls. Bonds was still living in Rwanda, where he was gearing up to analyze the data finally coming in to PIH, when the email from his brother-in-law arrived.
Bonds said he was too busy to get involved but would be happy to advise the Herrnsteins if he could enlist Michael Rich, a physician at Harvard Medical School who designed the health project in Rwanda.
Soon Bonds, Rich, and Jim Herrnstein were on a plane to Madagascar. They visited communities and toured health centers here, which were invariably depressing—dirty, poorly equipped, and distressingly empty. In one they saw a 6- or 7-year-old girl who was unconscious and near death. The health center lacked the intravenous malaria medicine Rich knew she needed, and her father could not afford $20 to rent a car to take her to the hospital 30 kilometers (km) away. Rich and her father rushed her there, only to find an empty emergency room and, again, no medicine. They drove to the nearest town and brought it back. The next day the girl had turned around. "It was dumb luck we were there and able to save her," Rich says. "We thought, why not always be there?"
In 2014, Rich and the three researchers founded PIVOT, with Bonds as CEO and director of research. Wright, Farmer, and Norton's father, conservation lawyer Edward Norton, serve on the board. PIVOT's first hire was Tara Loyd, a PIH veteran, who is now executive director. The Herrnsteins committed $5 million for the first 5 years. "The idea is we would give PIVOT a long runway," Jim Herrnstein explains, "so they will not be overly distracted by fundraising."
Shocking baseline data
PIVOT's office is a converted two-story stone house perched on a hill here a few minutes' walk from downtown Ranomafana. Its entire canvas is the Delaware-size district of 200,000 people, an 11-hour drive from Madagascar's brightly colored and terribly congested capital Antananarivo. Ifanadiana is dotted with some 1000 villages, with their distinctive houses of mud and thatch, connected by a maze of footpaths, and 14 towns. People here live off the land, and market stalls are piled high with pineapples, cassava, bananas, and rice.
Before PIVOT started any interventions, the team set out to gather a detailed snapshot of the health and socioeconomic conditions in the district. What they found would guide their efforts and serve as a benchmark to measure progress—and might ultimately help make the case that their system-wide approach is effective.
To design a baseline study, Bonds turned to his colleague, Harvard Medical School epidemiologist Ann Miller, who in turn teamed up with the National Institute of Statistics (INSTAT) of Madagascar. In April and May 2014, five INSTAT teams conducted face-to-face interviews at 1522 households, visiting each one three times to try to catch everyone living there. As part of the ongoing longitudinal study, INSTAT revisits the same households every 2 years.
The results were shocking. "We could see the district was poor, but we didn't know how bad until we got the baseline data," Miller says. In 2014, the study showed, one in seven children here never reached their fifth birthday. A woman faced a one in 14 risk of dying in childbirth. Both the maternal mortality and under-5 mortality rates were more than double the national estimate—and nearly twice as high as in sub-Saharan Africa as a whole.

In 2014, 81% of births took place at home, well above the national average of 57%—and only 20% were assisted by a trained midwife. Women here had an average of 6.9 children, as opposed to about five countrywide. Just one-third of children over age 2 were fully vaccinated. And although food scarcity is not considered a problem here, half the children were stunted, 21% severely so.
“Not rocket science”
When PIVOT started to work in the fall of 2014, it found a health system in tatters. A national plan calls for a three-tier system. For each fokontany, a cluster of remote villages with about 1000 people, the plan specifies two volunteer health workers. Each commune (there are 14 here) is supposed to have a primary health center staffed with three clinicians—a doctor, a nurse, and a midwife—as well as a pharmacy and a maternity ward, serving about 15,000. There is one hospital for the entire district. But when PIVOT arrived, almost none of that was functioning.
In the fokontany, community health workers were an infrequent presence at best, with little training and minimal or no supervision or support. The crumbling commune health centers looked like Soviet-era prisons and were about one-third staffed. If a patient made the long walk from the village and was lucky enough to find the center open, it was likely out of drugs because the pharmacist hadn't been paid and hadn't shown up. And the hospital, Bonds says, "was where you went to die."
PIVOT's strategy is to work with the government to shore up its system rather than impose its own vision of what a model health system should look like. That means, as much as possible, following government policies, although 4 years in project leaders are chafing at those limits.
"It's not rocket science," Robin Herrnstein says. "The biggest problems [killing children] are acute respiratory infections, malaria, and diarrhea. They are simple to treat. But you have to implement them all in one setting, and the second one piece breaks, you are done."
PIVOT made some district-wide changes right away—for example, hiring doctors and other staff at the 13 health centers and the hospital and training them in everything from obstetrics to infection control. Without PIVOT's intervention, "the health centers would be closed," says Andriamihaja Randrianambinina, who oversees health care here. They added an ambulance system and a team of social workers to help patients navigate the unfamiliar health system. The group also set up its extensive monitoring and evaluation program, collecting data from every remote health post, commune health center, and the hospital on every patient seen and cent spent.
Perhaps PIVOT's most important change was to remove all fees for patients at the three levels of care. Patients now receive medicines and treatment for free, and PIVOT reimburses the government. It is "incredibly cheap," Bonds says, costing just $0.90 per patient at the health center, and $10 at the hospital. PIVOT did this largely "under the radar," Loyd explains. "We didn't say we were doing universal health care—that would have been too threatening" at the time, she says. "But as we removed the cost of care, that is what we have been doing." Without PIVOT, Randrianambinina says, "the local people never would have been able to pay."
Then PIVOT focused on its first four communes of about 65,000 people, overhauling care at both the health centers and in the fokontany that feed into them. It plans to expand these efforts to all 14 by 2022.
Just getting to the remote villages from the road is a challenge. On a scorching day last May, a PIVOT team reached one of them after a sweaty, 2-hour hike on a slippery, narrow footpath that snaked over hills and descended into gullies so deep the mud sloshed over the tops of our boots. The only way across the many streams was to clamber gingerly across fallen tree trunks. It's hard to imagine how a woman in labor or someone feverish with pneumonia could make the trek to the health center. And many don't.
The two community health workers proudly show off their new one-room health post, painted cheerful blue and white. The health workers asked for someplace dignified to work, Bonds explains, so PIVOT supplies the building materials, and the community, the labor.
PIVOT and the Ministry of Health have trained the health workers in an international protocol for diagnosing and treating major childhood maladies. They now screen every child for malnutrition. Supervisors, a nurse or a midwife, visit each health post every 2 or 3 months to make sure the health workers are following the protocol correctly and provide refresher courses if not. They also collect the ledgers in which the health workers meticulously record each visit, test given, and drug dispensed—data that are fed into PIVOT's voluminous data base. Those data show that in the past 2 years alone, the number of sick children treated by the community health workers doubled. The main reason, the health workers say, is that care is now free.
But the people want more. As we are leaving, the village leader pulls Bonds aside and says the community wants a mobile clinic to visit once a month, a service PIVOT has provided in some villages. Bonds is sympathetic, but for now, PIVOT's hands are tied. The group has persuaded the government to provide clinics for villages 10 km or more from a health center, but this one is 9 km.
The group has also retooled the dysfunctional commune health centers. "This place used to look like a bombshell," Bonds says, gesturing around the Ranomafana health center, the first of the four to be upgraded. "People only came if they were deathly ill." PIVOT plastered and painted, added plumbing and latrines, and carted in solar panels. Today, the center is bustling, seeing 50 to 100 patients a day. Before PIVOT, there were two staff members. Now, there are 10 clinicians and two support staff.
Each health center now runs an outpatient feeding and treatment program for severe acute malnutrition (SAM), which can quickly become fatal. Each case triggers a home visit from the social team. "One case of SAM is an indicator of more suffering," Loyd explains.
The maternity wards have also been transformed. "Before, if you asked to see them, someone would have pointed you to a rusty bed with no mattress and no sterilized equipment," Loyd says. "Now, there is a real bed, with a mosquito net. Women have a place to sleep and recover with some dignity. There is a shower and food." When we visit one such ward, three young women are resting in bed with their swaddled newborns. They say they are thrilled with the care, but they also mention that the staff asked them for "a small gift." There is clearly more work to do.
Glitches aside, in PIVOT's first 2 years, the number of women delivering babies in health care facilities jumped 63%. Use of health centers for most other types of care tripled.

At the Ifanadiana District Hospital—the third tier of the district's health system—a tiny girl with enormous eyes shyly follows the visitors around the new malnutrition ward. She's a big success story: Admitted 21 days ago, she is almost ready to go home. PIVOT managed to convince a skeptical government that malnutrition was so severe that the hospital needed a dedicated ward. "We showed them the data," Loyd recalls.
In other ways, however, the Ifanadiana District Hospital has proved more recalcitrant. "The hospital is a puzzle to me—why the beds are not filled," Loyd says. PIVOT has built housing so that family members no longer have to sleep outside, renovated the emergency room, and built an isolation ward and a sophisticated diagnostic lab. Between 2014 and 2017, the number of hospital visits surged from 3116 to 5994. Yet still far too few patients come, and when they do, they often come too late or leave too early. "We thought [after removing fees] we would be scrambling for space, two people to a bed," Loyd says. "Instead, we have two or three people in a ward that can hold 10. … Is it something in the system? The quality of care?"
To Loyd, "The problems are all about remoteness and how to build trust in a system where people traditionally went to die. … Rebuilding trust takes years." Another factor, says PIVOT Country Director Mohammed Ali Ouenzar, is the rural population's long reliance on traditional healers and ancestral medicine.
The next day, Fara Rabemananjara, who heads PIVOT's team of social workers, takes us to visit a child who left the hospital too early. Three-year-old Charlindo had been admitted 4 months earlier with SAM and fever. His young mother brought him home before he finished treatment—possibly because the family had to work the cassava fields 16 km away. He was admitted again with SAM, typhoid fever, tuberculosis, and severe pneumonia. Recently discharged, the boy is getting weekly checkups at the hospital and at home.
The tiny wooden shack where he lives with his mother, grandmother, and three other children is a short walk through an alley, where the stench of sewage is unavoidable. All six family members share one bed, and the family ekes out a living on $2 to $3 a day.
Rabemananjara says she is thrilled with how well the boy looks—he has gained almost 1 kilogram since the last visit. To those who haven't seen him before, however, he looks anything but well. He is stick thin and, more troubling, lacks eye contact and any expression.
Intractable geography
PIVOT published the results of its longitudinal assessment, chronicling progress between 2014 and 2016, in June 2018 in BMJ Global Health, 1 month after a study from PIH documenting the impact of its Rwanda program between 2005 to 2010. Bonds and Rich, coauthors on both papers, argue in an editorial that the two projects provide some of the strongest evidence yet that strengthening the health system, rather than taking the piecemeal approach that donors favor, can go far in improving the health of the entire population.
In the area where PIH worked in Rwanda, under-5 mortality fell nearly 13% per year between 2005 and 2010. During PIVOT's first 2 years, the annual decline was almost 9%. These gains were achieved at a cost of just $30 per capita, despite Madagascar's low economic growth, political volatility, corruption, and scanty health spending. That, say Bonds and Rich, is proof that the Rwanda experiment is indeed replicable in less fortunate places. Bonds says: "If you can do it here, you can do it anywhere."
So far, so good
Key population health indicators for Ifanadiana district in Madagascar show progress toward ambitious goals.
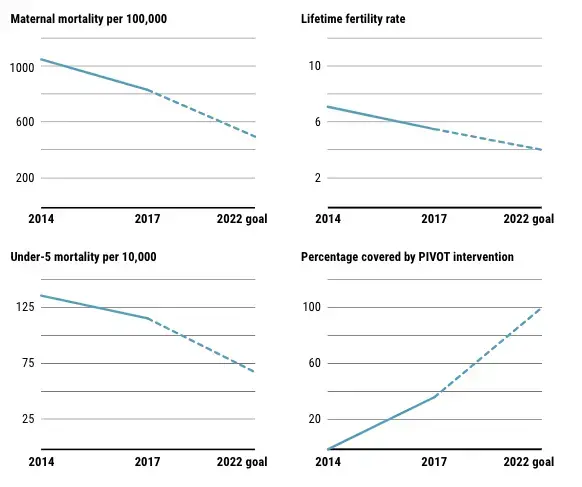
PIVOT researchers are now analyzing the results from year four. They expect to see a steady, positive trend. But as they put a finer lens on the data, they are finding that one problem has remained intractable: geography. "We have a large impact on people who live within 5 km of a health center, but a much smaller impact on people 5 to 10 km from a health center, and zero over 15 km," Bonds says.
The solution, PIVOT leaders say, is to bring more health services to the remote communities rather than the other way around. But they face two huge obstacles: Under the national health strategy, community health workers are unpaid volunteers, and they are not allowed to treat anyone over age 5—the rest must somehow make their way to a health center. "We are leaving the remote population behind," Bonds says. "Kids 6 or 7 are not getting treated and not making the trek. Why can't we treat a 6-year-old with malaria?" And, he adds, "You can't have untrained volunteers be the basis of your health system."
Global momentum is building to strengthen community health worker programs and ensure they are paid a decent salary. At a United Nations–sponsored meeting in October 2018 in Astana, Kazakhstan, World Health Organization member states committed to provide primary care for their citizens. Governments would be hard-pressed to foot the bill, but PIVOT and others believe the international community can help.
To see what is possible, PIVOT is piloting a new community health worker program in one of the 14 communes. "We want to get people better trained and pay them more—to professionalize them, so their scope of work can grow a lot" and they can treat older children and adults as well, Bonds says. Recently, the Malagasy government asked PIVOT to be the public face of its new push for universal health coverage, holding up Ifanadiana as a model for the nation. "The scaling up of PIVOT's effective and efficient intervention is a model for our journey towards universal health coverage," said then–Minister of Health Yoel Rantomalala.
PIVOT continues to expand. Since 2014, PIVOT's staff has grown to 182, 171 of them Malagasy, making it the largest health NGO in Madagascar. It is now covering about 95,000 people in seven communes—including Ambohimanga du Sud, reachable by an 8-hour tractor ride from Ranomafana—and is moving into its eighth. "The general idea," Loyd says, "is to remain nimble, keep a presence in Ifanadiana, and try to bring health care to the rest of the island. … We've got 24 million [people] to go."
The group's yearly budget has swelled to $4 million, and other funders have come on board. The Herrnsteins remain the largest donor, and say they are in it for the long haul. Robin Herrnstein says, "We have no exit plan and no plan to have one."