Story
 December 2, 2013
December 2, 2013
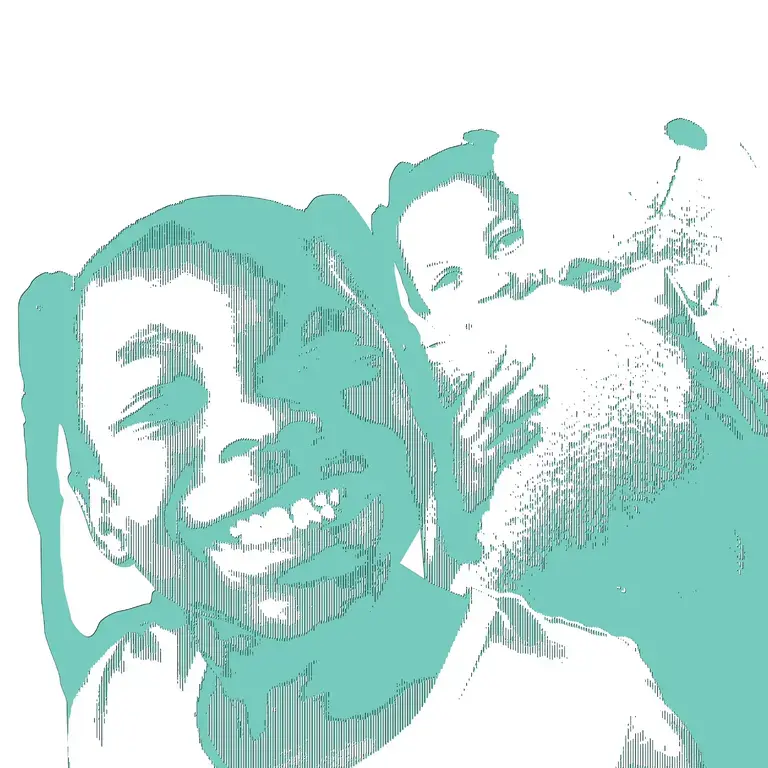
Mali: Desperate Situations Bring Back Old Malaria Interventions
Country:


Several African countries are preemptively treating children for malaria after trials found the...






An abandoned measure in malaria prevention has been resurrected in six African nations this year. About 1.2 million healthy children are swallowing malaria drugs to prevent the disease during the rainy season in regions where malaria mainly strikes within those months.
Fifty years ago, public health officials stopped administering antimalarial drugs to massive numbers of people in malaria-endemic areas because it leads to drug resistance, and also it's complicated to implement. Yet the strategy is making a comeback out desperation. Despite bed nets, insecticides and treatment, about 600,000 children die from malaria each year in sub-Saharan Africa.
As Humanosphere reported last April, Robert Newman, director of the malaria program at the World Health Organization (WHO), stressed the instability of malaria control. "If we let the pressure off," Newman said, "the disease will spring back." To keep that coil compressed, health workers administered malaria drugs prophylactically in parts of Mali, Togo, Chad, Niger, Nigeria and Senegal.
The version of mass drug administration that the WHO recommended last year — called seasonal malaria chemoprevention or SMC — will not work in East and South African countries where resistance to the medicines SMC uses, SP (sulphadoxine and pyrimethamine) and amodiaquine, is already widespread.
Grant Dorsey, a malariologist at the University of California in San Francisco who works in Uganda, is studying a more controversial version of chemoprevention based on the only compound that kills malaria parasites reliably around the world, artemisinin. Widespread artemisinin resistance would be catastrophic because there are no alternative cures. Yet Dorsey says, "We don't feel like we have another choice. Kids get malaria six times per year in Uganda, so as it is, they already take artemether/lumefantrine," an artemisinin-derived drug, often. "It's a desperate situation."
Just a few years ago, health officials might have held out for the "RTS,S" malaria vaccine — ten years and $550 million in the making. But recent results found that at very best, it is temporarily 56% effective. In contrast, clinical trials on SMC reported 75% to 86% (The Lancet) fewer malaria cases and deaths compared to control groups.
Badara Cisse, a malariologist at the University of Dakar in Senegal who helped lead the largest clinical trial for SMC says, "A malaria vaccine with 86% efficacy might win the Nobel Prize."
That efficacy will wear off eventually as parasites that resist SP and amodiaquine spread. I wrote about the ways that SMC is designed to slow that fate in a feature published last week in Nature. For now, however, the most pressing hurdles for SMC are logistical and financial. These were the challenges I noticed on my visit to Mali and Senegal in September.
In fact, I had initially intended to visit only Senegal in order to observe the largest rollout of SMC slated to occur there. With $1.5 million from the US Agency for International Development (USAID), the Senegalese government expected to reach 600,000 children, once each month, beginning in July. Yet the drugs did not arrive until October, so I headed to Mali where SMC occurred on time. It's not clear who to blame for Senegal's delay, suffice to say that neither the Senegalese nor the US government expected drug procurement to take as long as it did.
In Mali, Chad and Niger, Doctors without Borders (Medecins Sans Frontieres) reached a total of 440,000 children on a strict monthly schedule. They began SMC last year, and will continue at least through 2014. As an organization that prides itself on logistical prowess under duress, the group pulled off four rounds relatively smoothly.
Last year in Mali, SMC reduced childhood hospital admissions by 70% compared to the year before. This year in Mali, Bénédicte Lecoq, a field coordinator for Doctors without Borders, says that one of the rooms for children at the district hospital in Koutiala closed because it was uncharacteristically empty. I spoke with village chiefs, health workers and mothers, asking about side effects, the hassle of the intervention, and the potential for resistance, but I couldn't find a negative opinion of SMC. Instead, they were relieved to not struggle for the funds to take sick children to clinics.
However, for the program to work large-scale and long-term, MSF cannot guide the way, procuring drugs, and paying, training and supervising fleets of community health workers. Hospitals tend to be understaffed and under-equipped throughout sub-Saharan Africa, so there are few – if any – existing systems to draw from.
After my feature ran, Aleksandra Misiorowska, the associate director of the Malaria Medicines Venture in Geneva, emailed me to say that worries about drug resistance paled in comparison to more immediate concerns about the sustainability of SMC. She suggests that countries should try to work the intervention into existing community-based programs, and give those programs adequate support to take on a new function.
Doctors Without Borders attempted to do just that in Mali by combining the intervention with a nutritional program because more than a quarter of Malian children are moderately to severely underweight. When children came for their malaria pills, health workers would also measure the width of their upper arms. The organization hopes this dual-purpose will ultimately make SMC more cost-effective, and therefore more attractive when the Malian government looks to fund and organize it on their own.
In Senegal, health officials hope SMC will go smoothly because vitamin and vaccination campaigns already involve health workers visiting villages, as opposed to villagers reaching clinics. "We have a long history of door to door campaigns here," says Debbie Gueye, a malaria advisor at USAID in Dakar.
If SMC makes a significant dent in malaria over the next couple of years, it may trigger a revival of drug-based prevention schemes. Recently, the WHO recommended that HIV-positive people in sub-Saharan Africa take the tuberculosis drug isoniazid to prevent the disease. And last year, the US Food and Drug Administration gave their stamp of approval to preventative doses of an antiretroviral drug, Truvada, for healthy people at high risk of HIV. In order to deliver these interventions in Africa, countries must build a carefully orchestrated system of health care workers who can be equipped, supervised and paid to reach millions of people.
That might not be impossible. Several African governments have embraced projects like the One Million Community Health Workers Campaign, which aims to find village-elected health workers and provide them with the finances and tools they need to serve their communities. And malaria control officers in Mauritania, Burkina Faso, Gambia, Guinea Bissau, Cameroon and Ghana are scrambling for funds from USAID, UNICEF, and other organizations so that they can launch SMC campaigns next year.

Education Resource
Amy Maxmen on Malaria Prevention in Mali
In 2013, more than one million African children repeatedly took malaria medicines to prevent the...