



Two years after Euromaidan, the Russian seizure of Crimea and conflicts in eastern Ukraine, a...


On a rainy day last fall, longtime AIDS activist Olga Palamarchuk took me back to her new home in Odessa, Ukraine. To call it a home might be too generous; it was a chilly basement room in a halfway house for recovering drug users. But Olga and her teenaged daughter were happy to have a roof over their heads, two years after they fled Donetsk, a center of the war between Ukraine and Russian-backed separatists in the eastern part of the country. Olga is one of the estimated 1.7 million people displaced by the conflict. She participated in the massive demonstrations at Kiev’s central square, Maidan Nezalezhnosti, in 2013 and 2014, and in local pro-Maidan protests in Donetsk, where she was severely beaten by titushki, or paid thugs. Soon armed men — supporters of the Russian-leaning, anti-Maidan separatist movement — were shooting and beating whomever they pleased. “I was able to laugh at the explosions,” Olga told me, “but when the fighting started on my own street, I knew I had to leave.” Olga and her mother caught the next-to-last train out of Donetsk; Olga’s daughter had already departed.
Olga’s flight from Donetsk, where she had spent most of her life, was not the first dramatic rupture she had experienced. She learned that she was HIV-positive in 1997, when she was eight months pregnant. Not long after, she went into labor and called an ambulance; when she told the dispatcher about her HIV status, they refused to pick her up. She called again from a neighbor’s house, this time waiting to disclose her status until she was already inside the ambulance. In the maternity hospital, she was called a drug addict, though she didn’t even smoke cigarettes, and a prostitute. She was told that no one would help her, that no one would touch her, though she’d brought gloves and other protective items for the doctors to use. (It remains commonplace for patients to bring their own basic medical supplies with them to the hospital.) She gave birth with minimal medical assistance, after a failed attempt to escape to her mother’s house. The doctors were taken aback when her newborn daughter was healthy; they seemed to have expected a monster. Still, they said, the baby was sure to die in three years at most. The staff broadcast her HIV status so that the whole hospital treated her like a pariah. Olga’s daughter was HIV-negative, but only by good luck; Olga had not received medical treatment to prevent mother-to-child transmission of HIV.
The two major instances of ostracism that have marked Olga’s life — the discrimination she faced after her diagnosis and her wartime departure from her home — also define the boundaries of her country’s post-Soviet struggle. The cruelty she experienced in the hospital was typical for both Ukraine and Russia in the 1990s, a hangover from the Soviet period, when those suffering from stigmatized diseases or addiction were treated as social undesirables or criminals. Olga’s trajectory in the years since her diagnosis, on the other hand, is a testament to Ukraine’s divergence from this Soviet-style approach, as it accepted Western aid and allowed the development of nongovernmental organizations that fought hard to protect the health and rights of their communities. Olga discovered a local organization, Club Svitanok, that united former drug users and HIV-positive people to provide health and social services to their community; before long, Olga was working there, too, her life profoundly changed.
But the war turned everything upside down. Driven from their homes, Olga and her colleagues at Svitanok, as well as other eastern Ukrainian HIV organizations, faced the possibility that all their hard work would be lost, that their communities would once again be stranded and highly vulnerable. In many ways, the separatists were fighting to make eastern Ukraine more like Russia. Meanwhile, the members of Svitanok were struggling for their dignity — and, in the most basic sense, for their lives.

In the 1980s, as the HIV epidemic ravaged communities around the world, the Soviet Union remained in denial. Soviet leaders, with their abiding faith in the world-shaping power of propaganda, insisted that AIDS was a disease of decadent capitalists and third-world Africans; it couldn’t happen in the USSR. Suppressing information about drug users and gays, officials convinced themselves, would prevent these groups from existing. Such tactics had the opposite effect, pushing vulnerable people into higher-risk activities while denying them access to health services or even basic information about HIV transmission.
Things were no better after the Soviet Union fell. The health system collapsed with it, and there were few resources available — and little political will — to start the HIV testing, prevention, and treatment programs that were expanding in the West. Only when significant numbers of pregnant women and conscripts began testing positive did it become clear that Ukraine and Russia, the two post-Soviet countries hardest hit, were in the midst of a fast-moving HIV epidemic, spread largely by syringes shared during injection drug use. Even then, both the Russian and the Ukrainian governments were slow to respond, clinging to Soviet ideas about “socially unproductive” drug users and re-education through punishment.
But over time, the two countries diverged significantly in their approach to HIV and drug use. As Russia moved from the chaos of the 1990s to the authoritarian hold of Vladimir Putin, it doubled down on a firmly anti-Western, Soviet-style approach to HIV. Russian drug users were put on police registries and denied HIV treatment, sometimes placed in the same psychiatric institutions that had once functioned as prisons for Soviet dissidents. Opioid substitution treatment with methadone and buprenorphine, an effective form of HIV prevention for people addicted to opiates as well as an effective addiction treatment, was deemed a Western plot against Russia and forbidden. Needle exchanges that had opened in the late ’90s and early 2000s with the help of international aid organizations were threatened with legal action, their social workers branded “foreign agents.” Laws against “propaganda for homosexuality” made it dangerous to disseminate any kind of information about LGBT rights or health, and the government has tolerated, if not openly sanctioned, terrifying vigilante campaigns against the gay community, sex workers, and drug users.
Post-Soviet Ukraine, which was more open to international aid and advice than Russia was, took a different approach. Needle exchanges, methadone and buprenorphine programs, and targeted HIV services opened across the country. In comparison with Russia, Ukraine offered a more welcoming environment for NGOs and political advocacy, and local groups sprang up to work on HIV issues. In 1999, HIV-positive activists founded the All-Ukrainian Network of People Living With HIV/AIDS to advocate for their own rights and access to care. Those affected by HIV and drug use are often their own fiercest advocates, and the network grew to become one of the chief implementers of international grants for AIDS-related services, contributing to major progress in Ukraine’s response to HIV.
Although Ukraine’s HIV epidemic continues to grow, those affected have access to prevention, treatment, and support. Ukraine has substantially increased state funding for HIV treatment, and in November 2016, it announced that in 2017 it will fully finance the country’s program of opioid substitution treatment, which for the past 12 years has been supported by the Global Fund to Fight AIDS, Tuberculosis and Malaria. This puts Ukraine in even starker contrast with Russia, where doctors cannot even speak freely about substitution treatment.
Russia and Ukraine started in very similar situations, with crumbling, highly corrupt Soviet health systems, minimal knowledge about HIV prevention and treatment, and rampant HIV epidemics spread by injection drug use. Their contrasting responses to HIV are in many ways reflections of their differing understandings of their national identities and geopolitical positions. Longing to regain its superpower status, Russia under Putin has cultivated a sense of exceptionalism and an animosity toward the West. The Russian government rejects international aid, on the principle that such a great country doesn’t need outside assistance, and it rejects Western experience and expertise, on the principle that the Russian way is always better. It fosters a sense of paranoia — methadone is a conspiracy to enslave Russians, international aid is only a cover for espionage — even as it refuses to take basic steps to protect the health of its people.
Ukraine, on the other hand, has never had any pretensions to being a superpower. In a weak economic position, sandwiched between Russia and the EU, Ukraine has walked a fine line, trying to maintain its independence while also acknowledging that it needs help. It has actively solicited international aid (and sometimes squandered it, given its extremely high levels of corruption), and it has accepted the help of international experts, though reforming the country’s health care system has been an uphill battle. Though the Ukrainian political system is profoundly dysfunctional, it has not seen the consolidation of authoritarianism in the way that Russia’s has. Though they face many challenges, organizations like the All-Ukrainian Network of People Living With HIV/AIDS are able to continue their work. From the perspective of people living with HIV and injection drug users, Ukraine’s weaker geopolitical status has been an advantage.
But geopolitical weakness also has costs. For the Russian government, Ukraine’s vulnerability has been an invitation to assert its military strength and cultural chauvinism. And since the start of the ongoing war, that has come at the expense of Ukrainians living with HIV.

In 2003, six years after receiving her HIV diagnosis, Olga finally visited the Donetsk AIDS Center. There, she met a social worker from the local self-help group Svitanok (“dawn” in Ukrainian), which was founded by HIV-positive activist Svetlana Moroz as a peer support group for drug users and people with HIV.
Moroz had started injecting drugs in 1995, as a teenager in Donetsk. She quit in 1998 with the help of a former drug user who had started a peer support organization in Kiev, and she soon decided to return to Donetsk and start a similar group of her own. Over time, Svitanok expanded to offer a wide range of public health and social services while also advocating for the needs of HIV-positive people and drug users. (Donetsk has one of the highest HIV rates in Ukraine and in Europe overall; it also has a serious problem with multidrug-resistant tuberculosis, which is much more prevalent among people with untreated HIV and among prisoners.) Olga was brought into the Svitanok fold, becoming a social worker. Her position wasn’t just a job — it meant membership in a tight-knit group of friends dedicated to helping each other and those like them.
When the Maidan protests began in the winter of 2013-2014, most of Svitanok’s staff members were strongly in favor. For AIDS activists, the choice between Russia and Europe was a straightforward one, the difference between living and dying. Svitanok staff therefore found themselves on the wrong side of the new border when separatists declared the Donetsk People’s Republic in the spring of 2014. They were soon scattered across various Ukrainian cities, finding refuge where they could.

Svetlana Moroz spoke about the experience at an Odessa forum for HIV-positive women last September. Fair-haired and big-eyed, she radiated grief as she described the unfamiliar forms of trauma that Svitanok’s staff had experienced: shelling, food shortages, martial law. (Her own husband had volunteered for a battalion at the beginning of the war and had spent months in separatist captivity.) “Another trauma was the loss of the organization we worked so hard to build — separation from our beloved colleagues,” Moroz said. “But we’ve found a way to keep the organization going, to keep supporting each other even though we’re so far apart.” They had already lost their homes and their old lives to the conflict; they weren’t willing to give up on the organization that they’d worked so hard to build or on the progress they’d worked so hard to achieve.
Most of Svitanok’s clients remained in Donetsk, without the means necessary to leave in the long term. According to Natalia Bezelieva, Svitanok’s director, clients have been beaten, locked in basements, or forced to work for the separatists, packing sandbags for barricades. Some have been forced to loot damaged or abandoned houses.
As far as HIV and drug policy is concerned, “it’s like going back in time 10 years or more,” Bezelieva told me. The Donetsk People’s Republic modeled its HIV “policy” on Russia’s — which is to say, there was virtually no provision of medical support to those affected. Bezelieva told me a “half-partisan” harm reduction program is still operating in Donetsk, with workers paid secretly to distribute syringes and condoms. (There are a number of such programs in Donetsk and Luhansk.) The number of clients has increased dramatically; many are now homeless, without enough food or clothing. Families have been divided by the border, and there are higher rates of overdose from illegal drugs. Decreased access to medical treatment has coincided with an increase in the availability of opiates, according to Svitanok staff, with much larger quantities of illicit methadone slipping across the porous border with Russia (ironic given that medical methadone is illegal there) and easily available opium made from poppies grown in abandoned fields. In an atmosphere of arbitrary violence, deprivation, and uncertainty, opiates offer the afflicted relief, however self-destructive.
Members of Svitanok turned their energies to resistance. By January 2016, they concluded that a covert system of medical shipments would be necessary for the Donetsk People’s Republic. The territory was about to run out of antiretroviral drugs, risking a dangerous treatment interruption for HIV patients there, including children. Patients with tuberculosis — in many cases, difficult and deadly multidrug-resistant tuberculosis — faced the same problem. It was clear that international organizations like the Global Fund and UNICEF would not be able to arrange for an official shipment in time.
Svitanok decided they would need smugglers, all of whom would be women. It wasn’t just that women have long been at the forefront of Ukrainian activism; they had certain advantages in this kind of clandestine work. Because they are so widely dismissed in Ukraine, women can get into places men often can’t, can cajole border guards in a way that men cannot. (They are also more vulnerable. The conflict in Ukraine has resulted in a dramatic increase in gender-based violence, according to United Nations Population Fund, and the U.N. has reported acts of sexual violence committed with impunity by fighters on both sides.)
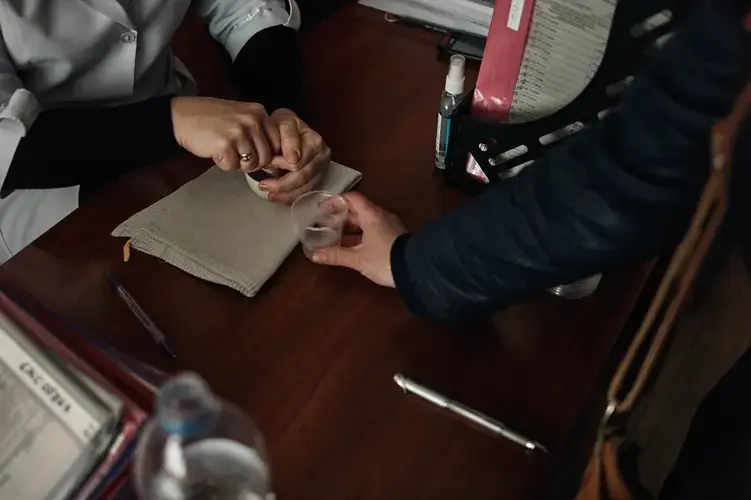
Among the first women to carry medicines across the border was a social worker named Irina (I have changed her name), traveling with two of her colleagues who had also remained in Donetsk. The three women drove back to Ukrainian-controlled territory and received a shipment of antiretrovirals from the All-Ukrainian Network of People Living With HIV/AIDS. A doctor had provided them with an official document saying that the medication in the car was for the personal use of the passengers; they knew they’d run into trouble if they stated honestly that they were bringing in medications for distribution.

When they had nearly reached the “gray zone” between Ukrainian-controlled territory and the Donetsk People’s Republic, Irina approached the Ukrainian checkpoint on foot, showing the guards her official documents. Unfortunately, the helpful doctor had listed the real cost of the medicine, although Svitanok had received it for free. Seeing the relatively high price, the guards demanded a bribe. Irina was able to pay it, and she and her colleagues continued across the gray zone.
On the other side, the Donetsk People’s Republic guards asked for an even larger bribe, one Irina couldn’t afford. Told she’d have to abandon her boxes of pills, she sat down and declared that she wouldn’t move until she was allowed to cross. “I have HIV,” she said, “and if you don’t let me through with my medicine, I’ll die.” Finally, she was allowed to go to a nearby village on the border and call the local AIDS center, which helped negotiate her passage.
On her next trip over roads pocked and torn by shells, past bombed-out buildings, Irina made sure her documents didn’t list the price of her contraband. The border guards gathered around her when she got out of her car and asked to speak to a person in charge; seeing a young woman, they assumed she was hoping to skip the line, perhaps with a bribe in hand.
They were bemused, though not particularly hostile, when she explained that she had HIV and tuberculosis. She made it through several checkpoints and multiple rounds of questioning, her face half-covered by a gauze mask. The border guards wore masks, too, for fear of contagion.

For all its deprivations, the Donetsk People’s Republic is enlightened compared with the Luhansk People’s Republic. Luhansk’s health policies are copied from Russia’s, and there is no evidence-based drug treatment or HIV prevention in the republic. The Luhansk People’s Republic is even opposed to condom distribution, advocating an ultra-traditionalist ideal of femininity even as the area’s economic devastation has made women more and more likely to have to trade sex for food. As in Donetsk, social workers who have remained in separatist-controlled Luhansk continue to provide underground health services, working even during shelling.
They also assist unlucky inmates stranded in prisons on separatist-controlled territory and the newly released who face an arduous journey to their homes on the Ukrainian side of the border. It’s not uncommon for people just released from prison to feel they’ve been transported into an unfamiliar future; Ukrainian prisoners released into the separatist republics find themselves in a kind of parody of the past. Rewind to the years before HIV-positive people were treated as patients, before drug users were considered to have a right to medical care. Rewind to Russia.
But the smuggling mission in Luhansk became significantly more arduous in the fall of 2014, when the government of the nascent People’s Republic entirely forbade the shipment of medicines, groceries, or other goods into its territory. Valeria Rachinska, a former sociologist from the Luhansk region who now works at the All-Ukrainian Network of People Living With HIV/AIDS, told me that on a trip during this period, she and her colleagues were accused of being special agents, saboteurs. They were interrogated and searched for five hours, the border guards emptying every box and bag, leafing through every piece of paper, checking inside tubes of toothpaste.
“We danced, we coaxed, we threatened, we cried,” Rachinska said, “but we made it across every time.… We were willing to do anything necessary to make sure that there would be antiretroviral treatment available on both sides of the line of contact.” On one occasion, they were told that they had only an hour to make it across the border before the shooting started again. After the single crossing point into Luhansk accessible to cars was bombed, at the end of 2014, Rachinska and her colleagues — again, almost all women — made the crossing by foot, carrying their precious cargo in suitcases, backpacks, or plastic bags, trudging alongside the many unhappy people who were making the long, dangerous trip to buy groceries or medicine or to collect their pensions on the Ukrainian side.
At one point, two of Rachinska’s colleagues went to deliver antiretrovirals to a prison in Krasnyi Luch, in separatist-controlled territory, during active fighting, when there was the risk that they would be hit by a shell or that they would drive over a mine. They succeeded in preventing a treatment interruption for the prisoners. “Two skinny girls, each weighing about 45 kilos, were able to do what a whole government couldn’t,” Rachinska said.
This illicit method was dangerous and allowed for only small shipments; even when supplemented by occasional interventions by NGOs like Médecins Sans Frontières (MSF), it clearly had to be replaced by a more formalized system. But Ukrainian AIDS activists and international aid agencies had great difficulty persuading authorities in Kiev and the separatist enclaves to agree on a plan. On the Ukrainian side, the government was doing its best to maintain a blockade, which it hoped would starve the separatists into submission. Hard-liners argued that anyone who stayed in the separatist-controlled areas was a traitor and didn’t deserve any kind of help. (In fact, many had remained because they had little choice, being disabled, elderly, or poor, or caregivers for family members or friends who couldn’t leave.) In the summer of 2015, the Security Service of Ukraine introduced a system of checkpoints to control access to the separatist-controlled areas, severely limiting legal opportunities to deliver medications. During this period, activists carrying medicine across the gray zone were risking double punishment. They continued to make the trip, nonetheless.
The Global Fund eventually provided an emergency grant of $3.6 million to UNICEF, which was able to negotiate medical shipments into the Donetsk People’s Republic starting in August 2015. They succeeded in winning the cooperation of the Ukrainian government, which adopted a more humanitarian approach to the separatist-controlled zones, despite pressure from nationalists to renew the blockade. Irina, from Svitanok, told me that when she transported a shipment of medicines in September 2016, the Ukrainian border guards were honest and sympathetic. The last of five antiretroviral shipments was completed in November 2016, providing enough medication to last until mid-2017, when another shipment is planned. The Global Fund has approved a grant that will provide medicines through mid-2018. After that, the future is uncertain. Ukraine’s economy is in a perilous state, and in an era of growing austerity and isolationism in the United States and Europe, international aid is always at risk.

By the end of 2017, an estimated 12,500 patients in separatist-held Donetsk and Luhansk will be in need of HIV treatment. The current arrangement is only a short-term solution. According to Michel Kazatchkine, the U.N. secretary-general’s special envoy on HIV/AIDS in Eastern Europe and Central Asia, given that the conflict is unlikely to be resolved in the near future, the most viable longer-term solution may be to include an arrangement for funding of HIV and drug-resistant tuberculosis treatment in the international negotiations that have arrived at two (largely unsuccessful) Minsk agreements for cease-fires and roadmaps for an end to the conflict. “If no solution is found in the coming months,” Kazatchkine wrote in a recent comment in The Lancet HIV, “the region may again be at risk of treatment interruptions for HIV and drug-resistant tuberculosis that would lead to a regional public health crisis.”
Unfortunately, the rapidly changing political situation in Ukraine, Europe, Russia, and the United States makes such agreements more tenuous than ever. (Cease-fire agreements have been routinely violated by both sides in the conflict.) The separatists are capricious and could withdraw their permissions to UNICEF at any time; they have expelled many of the humanitarian groups that have operated on their territory, including MSF. The UNICEF shipments do not provide tuberculosis medications or laboratory supplies; activists continue to transport these informally and to carry blood samples in refrigerated containers back to Ukrainian labs for diagnostic tests unavailable in separatist territory.
After a lull, such trips have again become more dangerous. A surge in fighting began in January; opinions differ as to whether this was Ukraine’s attempt to make inroads before newly elected U.S. President Donald Trump changed the political calculus, a Ukrainian bid for Western assistance, or a strategic move by a Russia emboldened by Trump’s election. In late January, Ukrainian nationalists began an informal and illegal physical blockade of railway lines used to transport coal and other industrial goods between the separatist-controlled areas and the rest of Ukraine. In response, separatist leaders took control of Ukrainian-owned coal mines and steel mills on their territory, vowing to sell their products to Russia instead. Ukrainian authorities finally arrested some of the nationalist protesters in mid-March, but then Kiev officially stopped all cargo traffic with separatist-held areas, demanding that pro-Russian separatists return the Ukrainian businesses. All railway and road connections are to be cut until the separatists comply with Kiev’s demands. President Petro Poroshenko said only humanitarian cargo should be allowed to pass into separatist-held areas, but it remains to be seen how feasible this will be as relations between Kiev and the separatists become even more contentious.
The future of HIV and tuberculosis treatment in eastern Ukraine remains uncertain, but Ukraine’s AIDS activists are determined to do everything they can to save it. With their unwavering commitment to helping some of the most vulnerable people in society, even at great personal risk, these activists believe they are embodying the best of Western values. As the conflict wears on, one hopes the West will agree.

Education Resource
Meet the Journalist: Sophie Pinkham
Journalist Sophie Pinkham speaks about her reporting on the work of AIDS activists in eastern...


